adssx
#154
I can’t find data on the frequency. It seems extremely rare. So much that it might not be relevant at all.
What are sources about that? In Google Scholar I could only find:
Neo
#155
For me it is about triangulating between data and mechanistic understanding. The latter part is a very key part of my approach - even if the data, data, data is crucial, and mechanistic understanding in isolation is seldom good enough to make decisions based on.
We know with very high confidence that Apo B is *causal in increasing CVD. (More so than most relationships in medicine). So when I and my doctors and making decision about my CVD risk reduction protocol we are bringing to bear both “averages” data from clinical trials and Mendelian Randomization studies AND mechanistic understanding and then making triangulated decisions for me in my context with all the N=1 data we have for me.
3 Likes
Neo
#156
Do we know what the centenarians had as lipid levels when they were young and middle age? Seems that would be more interesting to know than what their levels are when they are very old (as we know that Apo B goes up with age).
We also need to know mechanistically that non low lipids (at old age) are helping them become old vs that they are becoming old despite
Otherwise we are just back in associations and correlations and not causation.
Don’t know details, but I’ve heard that centenarians have better reverse cholesterol transport than “normal” population - if so they may be genetically less sensitive to higher lipid levels.
2 Likes
scta123
#157
Does it have a strong prediction value as well?
Neo
#158
As mentioned before - I’m aiming at seeing if I can give it a shot to live healthily to 100-120 and perhaps beyond.
In that context my best estimate is that lower Apo B will decrease my risks of CVD in the later decades.
(If/as I experience any negatives or as new data and mechanistic understanding comes out I might/likely will calibrate along the way).
Not sure what is new here, so will engage less as long as it feels like just back in versions of past conversations here on the forum being rehashed.
3 Likes
cl-user
#159
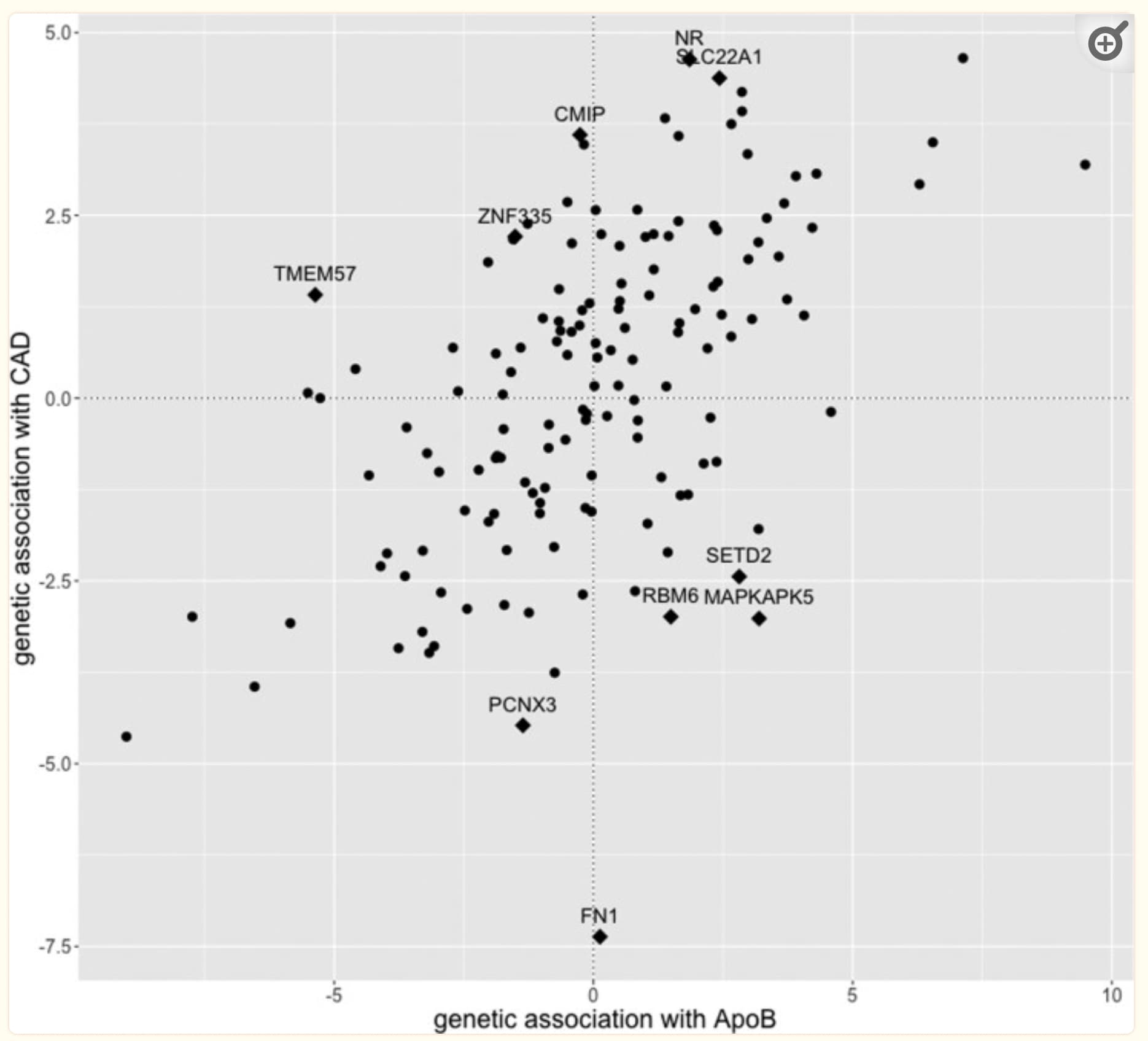
Nope: The causal effect is 0.464 (Model-averaged causal effect 0.392). Better than any other coronary artery disease (CAD) predictor they looked at though.
ApoB remained the highest ranking individual model (model posterior probability 0.455) and the risk factor with the strongest marginal evidence[…]
No alternative risk factor had similar strength of evidence, suggesting that ApoB is indeed the most important risk factor and not just a representative of a group of highly correlated lipoprotein measures with similar evidence. On exclusion of ApoB, the top risk factors were triglycerides content in small HDL particles (marginal inclusion probability 0.461, FDR <0.05) and LDL cholesterol (marginal inclusion probability 0.417, FDR <0.05). Yet, the evidence for these two lipoprotein measures is much weaker compared to the evidence for ApoB in the main analysis.
From: High-throughput multivariable Mendelian randomization analysis prioritizes apolipoprotein B as key lipid risk factor for coronary artery disease
They have some interesting takeaways:
ApoB has been shown to be a superior measure to LDL-cholesterol in the prediction of CAD risk and in prediction of coronary artery calcification. From a clinical perspective, statins target LDL-cholesterol levels rather than ApoB, suggesting that greater benefit might be obtained from lipid-lowering drugs that target lipoprotein particle number. When analyzing data from UK Biobank only, there was also some evidence for triglyceride content measures as an additional risk factor.
5 Likes
Neo
#160
Thanks for valuable share.
That seems like a very strong relationship for something in medicine?
From what you quoted above, it seems to me to be a “yes, relatively strong”
Edit: that seems be inline with (or weaker than) what the authors feel and state themselves:
5 Likes
adssx
#161
Also, this centenarian study only looked at total cholesterol. Until we have a study looking at apoB and HDL (or maybe even HDL quality and subtypes as suggested above) we cannot conclude much. (The CETP inhibitor trial results will be very interesting and will hopefully help us improve our mechanistic understanding…)
4 Likes
cl-user
#162
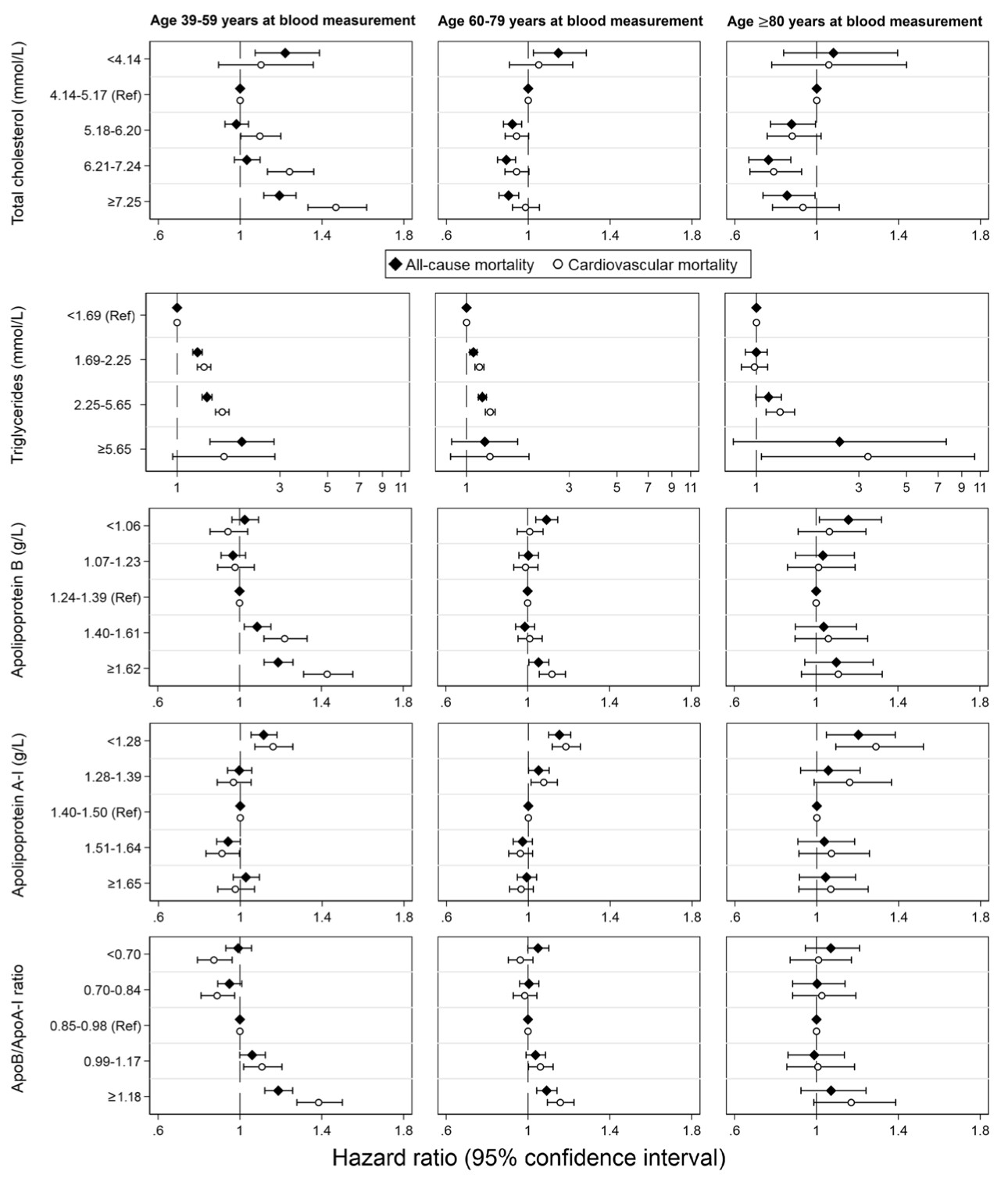
Here it is. This one is particularly interesting because it has CVD and all cause mortalities.
It is consistent with all the similar studies:
- High TC is only bad below 60 and good after 60.
- High APOB is bad below 60 and don’t care after 60.
- Very high APOB is very bad below 60 and slightly bad after 60.
- Very low TC and APOB are always bad or trending bad.
- High TG is always bad.
- Low APOA1 (HDL) is always bad.
From
The association of apolipoproteins with later‐life all‐cause and cardiovascular mortality: a population‐based study stratified by age
4 Likes
However if we expect to have longer lifespans than regular folks, we may want to keep ApoB and TG lower for longer.
4 Likes
cl-user
#164
it’s not what the plots show.
Very low TC is always bad for all cause mortality for all age groups.
Very low TC is trending bad for CVD mortality for all age groups though not statistically significant.
So if you have a too low TC you die sooner.
For APOB there is no significant effect for very low, low or medium levels.
Very low APOB is trending bad though not statistically significant.
High and very high APOB is bad.
So keep your APOB low of medium. Extremes are bad.
In all cases TG is bad and low HDL (APOA1) is bad.
L_H
#165
I think we can only say that very low TC is associated with por all cause mortality. It may or may not be bad.
3 Likes
cl-user
#166
Yes, that’s correct! These do not imply causality.
3 Likes
Sorry, I made a typo. I meant TG not TC. I agree with both of you.
LaraPo
#168
Actually your debates with youthful assertiveness ( ) were pretty educational for me. I learnt a lot. So, keep debating!
) were pretty educational for me. I learnt a lot. So, keep debating!
3 Likes
adssx
#169
Thanks.
But people with low ApoB probably have low TC as well?
Could it be that you want to minimize ApoB while maximizing some “good” cholesterol (that is probably more complex than just “HDL”).
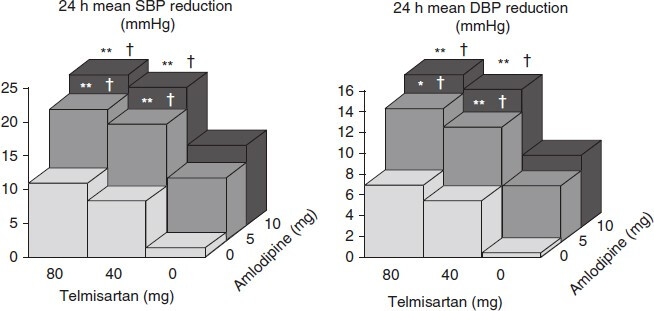
As I said earlier what I’d love to see is a two dimensional chart with ApoB and TC (or HDL or some HDL subtypes as it seems that quality matter).
Could be done in 3D like this:
3 Likes
scta123
#170
I believe that what matters most is the process of reverse cholesterol transport. It’s not just about the composition of HDL-C or quantity of apoA-1 particles, but rather the effectiveness of removing cholesterol from tissues. Unfortunately, this process cannot be easily measured and is not fully understood yet. Once we find a medical intervention to address this issue, then we can consider the end of ASCVD IMO.
3 Likes
adssx
#171
What makes you believe this?
2 Likes
Neo
#172
1 Like
adssx
#173
2016 paper with 0 recent citations: is there more recent progress in this field? (I don’t know anything about this topic)
1 Like