ng0rge
#278
My intention was in no way to minimize the importance of learning more about heart disease, it’s causes and potential solutions. My point was only that these threads sometimes seem to get bogged down in a loop, like a wheel spinning in the mud. I am still learning more (like how you can still have plaque buildup with a CAC score of zero) but want to use my time efficiently (it is limited, after all, for all of us).
5 Likes
Neo
#279
Thanks for the summary. There are some things I’d frame and explain differently for those three buckets (especially how MR in the context of CVD is stronger than in other areas*), but at a meta level if think the following might be more important to add:
-
while those three groups have some strengths and weaknesses there is a scientific consensus of a hierarchy of how valuable the data is from different types of studies and they are not ranked the same - in general association studies are massively weaker than MR and controlled clinical trials
-
perhaps even more important is that there is a massive wealth of mechanistic understanding of the cardiovascular disease process. CVD is one of the areas in medicine that we understand the most and the best. It’s not like Alzheimer’s or cancer. This includes all the in vivo animal studies and in vitro studies. While we don’t know everything the consensus is that we really do know that Apo B is causally involved and virtually a necessary conciliation for CVD. Yes, we also know that inflammation plays a role. That glucose plays a role etc. and decreasing each of those is valuable too.
I’m not saying people in general should make medical decisions based on mechanistic understanding and logic without data. Rather this is a case where the mechanistic understanding is stronger than in almost any other part of medicine - and it aligns basically perfectly with randomized trials, MR, animal studies.
The last thing I think might be missing from the framework is what we know about side-effects and risks. In the context of - what is the upside here (avoiding number 1 killer (heart) AND number 1 thing leading to real, severe disability (stroke). Again, Apo B lowering is one of the areas in medicine where we have the most info about that - and the risk/effects profile of the tools available is generally very favorable - especially if one applies @约瑟夫_拉维尔 ’s framework of quickly and broadly evaluating any adoption of a medicine and dial it in/up/down/out. For instance while statins are probably totally find for a majority of people, for some people they won’t be - but for almost of those case that will be clear from what the person experiences over the first days or weeks and/from blood work over the firsts weeks/months. Try and if not optimal move on and try something else.
Finally, while I know that some people don’t like Dr Attia (and I personally strongly disagree with him on some topics like about protein intake protocols, etc), his general framework of how we can and need to move from Medicine 2.0 to 3.0 seems very relevant here.
See for instance The evolution of medicine and the transition to “Medicine 3.0” from round 3min to 11min 45sec in link below
(Better covered in his book if I recall correctly)
6 Likes
A_User
#281
So you’re telling me @Neo that your standard of evidence isn’t one compiled by a Superintelligent Laplace demon?
Bicep
#282
I used to believe this, but now see it’s impossible. You can’t know both position and momentum of say an electron. You change things when you measure them. It’s not a matter of not being smart enough or not having a computer fast enough. It’s unknowable. I have no idea what’s actually going on but it seems more like a simulation all the time.
2 Likes
A_User
#284
This is the straw man. Recognize that I am saying the MR studies and RCT’s specifically about apoB in context, not the methodology in general. Meaning I am waiting to hear someone question the specific RCT’s or MR studies that have been posted a gazillion times. Different studies have worse or better methodologies. To reject RCT and MR as a whole basically means someone is a quack, psuedoscientist, lysenkoist, whatever label fits.
2 Likes
All of the above is true and well explained but it seems some people have difficulties grasping stochastic processes and view the curves as deterministic which they are not.
BTW as an example of MR, I’ve posted about an MR study about the causality of APOB for CAD and indeed there is some causality but much less than people think: The causal effect is 0.464 (Model-averaged causal effect 0.392). Better than any other coronary artery disease predictors (LDL, etc.) they looked at though but still rather weak.
2 Likes
Neo
#287
@cl-user do you have any comments on my reply to your post on this?
adssx
#288
@A_User I know you’re honest in defending your views (and I somewhat agree with them) but, as I cannot send you an MP, just to remind you that writing in bold + all caps is like shouting. In addition to being rude, it is counter-productive (assuming that your intent is to convince others): your “opponents” in this debate won’t be convinced by the same arguments (otherwise they would have changed their mind long ago) and “neutral” readers/lurkers (the silent majority) can be repelled (as I was initially) and prefer to “side” with the seemingly more rational and peaceful participants than with the religious zealot yelling at others.
7 Likes
Who said anything about rejecting them? It is not a black and white world.
1 Like
A_User
#290
As long as people understand that the pro-position is based on clinical trials. We should debate the science.
I don’t know if there are any better studies except this one. Or if there are any clinical trials with the opposite result. The latter is what I asked for in general.
3 Likes
ng0rge
#291
First, I think we should focus on ApoB-I think it’s a better marker- and in your case, I think the sight of “LDL” is like waving a red flag in front of a bull. On ApoB, I agree with you that lower is better-the science to me is clear. Now if you are saying everyone should keep working until their ApoB is 20, that seems irrational.
Reading your posts…the words didactic, pedagogue, pedantic (I didn’t say borderline psychotic  ) come to mind. The bigger issue is not so black and white. When you add in personal circumstances and individual biochemistry (genetics, etc) there are lots of reasons that people may chafe at being lectured about lowering ApoB.
) come to mind. The bigger issue is not so black and white. When you add in personal circumstances and individual biochemistry (genetics, etc) there are lots of reasons that people may chafe at being lectured about lowering ApoB.
You do get extra points for using “lysenkoist”, I’ve added that to my list of things I love about the Russians ( along with the picture of a bareback Putin on a bareback horse and their colorful behavior drinking vodka).
L_H
#292
I agree.
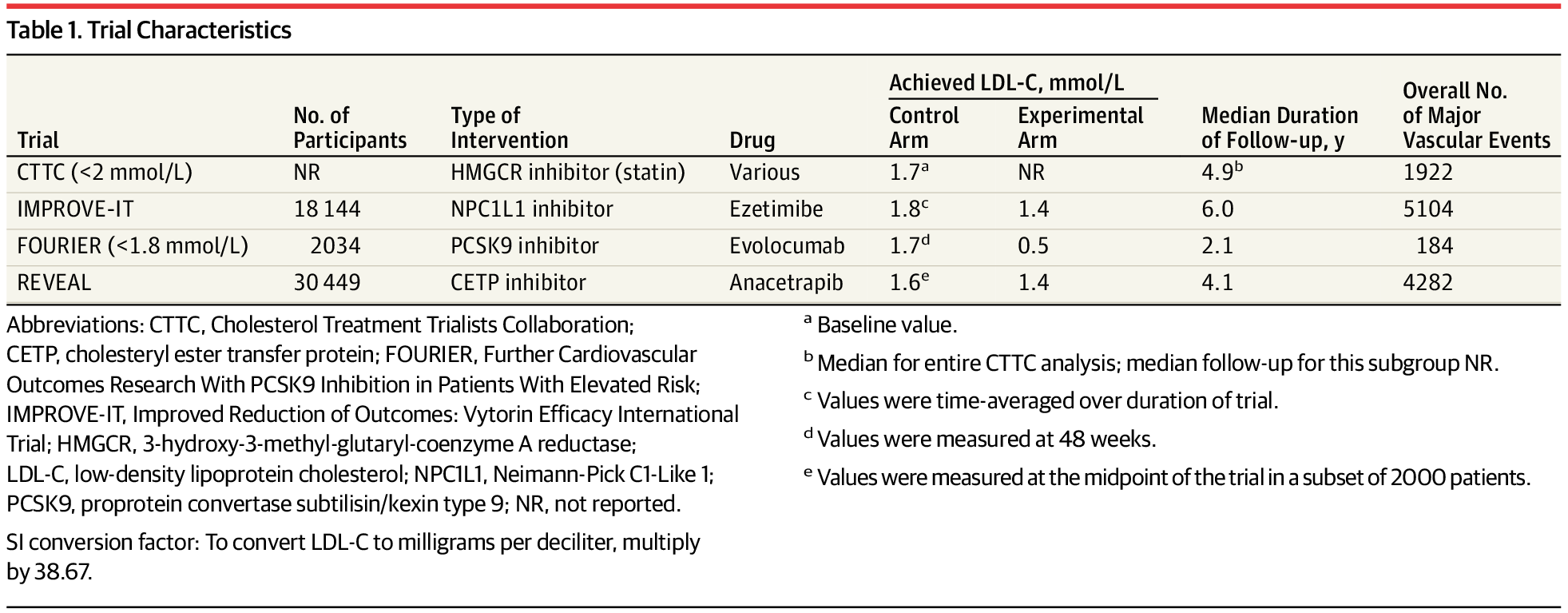
This is a decent meta analysis of rcts, but i think it illustrates your point.
it only looks at secondary prevention, so in people who have already had a heart attack etc . And the studies are short term.
For anyone who has had an MI or stroke, getting apob as low as possible looks like a good bet. The long term is less of a concern and preexisting atherosclerosis (and preexisting risk factors for atherosclerosis) means the body is less able to deal with inflammation, oxidized non-hdl lipid particles etc.
But it’s a big leap to generalize this to decades long use of pharma in healthy, low inflammation, low oxidation individuals. We have no real way of quantifying either side effect risks or benefits from going from low to extremely low.
ng0rge
#293
Again, I would focus on studies that use ApoB and not…uh…you know…(careful, I hear snorting)… But with ApoB, I think that it’s good, sound, general advice (apart from individual complications) to aim for lowering your ApoB to say 50 or so (maybe even 40-50) if you don’t have to go to uncomfortable lengths to do so.
ng0rge
#295
Hey! I have a Pope’s hat in my closet…but I only pull it out when I’ve had too much coffee (why should only the Pope have all the fun??)…besides, it scares my cat.
2 Likes
A_User
#297
LDL is almost the same thing as apoB.
It is not my decision how much someone should smoke.
ng0rge
#298
Hold on, let me get my bot (not named vlasko) to start firing off studies about why ApoB is a better measure than LDL…cuz we all know it is.
ng0rge
#299
Here’s a carefully hand-picked article that is short and to point (but nothing new).
“If the amount of cholesterol per particle was always the same, measurements of your cholesterol values (LDL-C and non-HDL-C) and your particle numbers (LDL-P and ApoB) would give very similar results. However, because the amount of cholesterol carried inside lipoprotein particles is highly variable, cholesterol tests and particle number tests frequently show conflicting values with regard to your cardiovascular risk. In statin intervention trials, apoB levels on therapy are a significantly stronger predictor of cardiovascular event reduction versus LDL-C or non HDL-C. Your LDL-P and ApoB particle score is your best reference point to track your cardiovascular risk.”
https://precisionhealthreports.com/ldl-p
1 Like
A_User
#300
I said almost the same thing. ApoB is superior, of course.