A_User
#290
As long as people understand that the pro-position is based on clinical trials. We should debate the science.
I don’t know if there are any better studies except this one. Or if there are any clinical trials with the opposite result. The latter is what I asked for in general.
3 Likes
ng0rge
#291
First, I think we should focus on ApoB-I think it’s a better marker- and in your case, I think the sight of “LDL” is like waving a red flag in front of a bull. On ApoB, I agree with you that lower is better-the science to me is clear. Now if you are saying everyone should keep working until their ApoB is 20, that seems irrational.
Reading your posts…the words didactic, pedagogue, pedantic (I didn’t say borderline psychotic  ) come to mind. The bigger issue is not so black and white. When you add in personal circumstances and individual biochemistry (genetics, etc) there are lots of reasons that people may chafe at being lectured about lowering ApoB.
) come to mind. The bigger issue is not so black and white. When you add in personal circumstances and individual biochemistry (genetics, etc) there are lots of reasons that people may chafe at being lectured about lowering ApoB.
You do get extra points for using “lysenkoist”, I’ve added that to my list of things I love about the Russians ( along with the picture of a bareback Putin on a bareback horse and their colorful behavior drinking vodka).
L_H
#292
I agree.
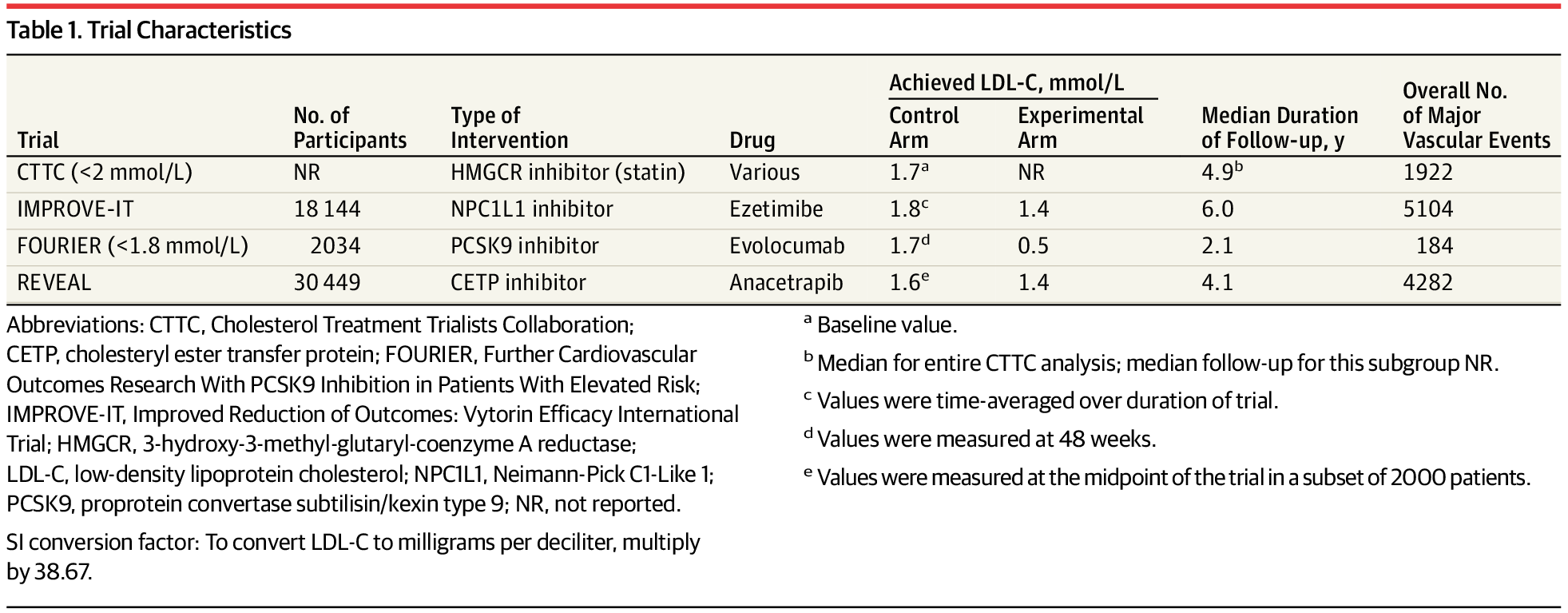
This is a decent meta analysis of rcts, but i think it illustrates your point.
it only looks at secondary prevention, so in people who have already had a heart attack etc . And the studies are short term.
For anyone who has had an MI or stroke, getting apob as low as possible looks like a good bet. The long term is less of a concern and preexisting atherosclerosis (and preexisting risk factors for atherosclerosis) means the body is less able to deal with inflammation, oxidized non-hdl lipid particles etc.
But it’s a big leap to generalize this to decades long use of pharma in healthy, low inflammation, low oxidation individuals. We have no real way of quantifying either side effect risks or benefits from going from low to extremely low.
ng0rge
#293
Again, I would focus on studies that use ApoB and not…uh…you know…(careful, I hear snorting)… But with ApoB, I think that it’s good, sound, general advice (apart from individual complications) to aim for lowering your ApoB to say 50 or so (maybe even 40-50) if you don’t have to go to uncomfortable lengths to do so.
ng0rge
#295
Hey! I have a Pope’s hat in my closet…but I only pull it out when I’ve had too much coffee (why should only the Pope have all the fun??)…besides, it scares my cat.
2 Likes
A_User
#297
LDL is almost the same thing as apoB.
It is not my decision how much someone should smoke.
ng0rge
#298
Hold on, let me get my bot (not named vlasko) to start firing off studies about why ApoB is a better measure than LDL…cuz we all know it is.
ng0rge
#299
Here’s a carefully hand-picked article that is short and to point (but nothing new).
“If the amount of cholesterol per particle was always the same, measurements of your cholesterol values (LDL-C and non-HDL-C) and your particle numbers (LDL-P and ApoB) would give very similar results. However, because the amount of cholesterol carried inside lipoprotein particles is highly variable, cholesterol tests and particle number tests frequently show conflicting values with regard to your cardiovascular risk. In statin intervention trials, apoB levels on therapy are a significantly stronger predictor of cardiovascular event reduction versus LDL-C or non HDL-C. Your LDL-P and ApoB particle score is your best reference point to track your cardiovascular risk.”
https://precisionhealthreports.com/ldl-p
1 Like
A_User
#300
I said almost the same thing. ApoB is superior, of course.
ng0rge
#301
This study is also interesting. - “Discordance between LDL-C and Apolipoprotein B Levels” - They divided the study participants into 4 groups with LDL-C and ApoB scores.
“group 1 (low LDL-C, low ApoB), group 2 (low LDL-C, high ApoB), group 3 (high LDL-C, low ApoB) and group 4 (high LDL-C, high ApoB).”
Particularly see group 3, even with high LDL-C, it’s the low ApoB that accounts for a good outcome.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8781725/
1 Like
Sorry. Missed it. Here it is.
1 Like
Neo
#304
3 Likes
adssx
#305
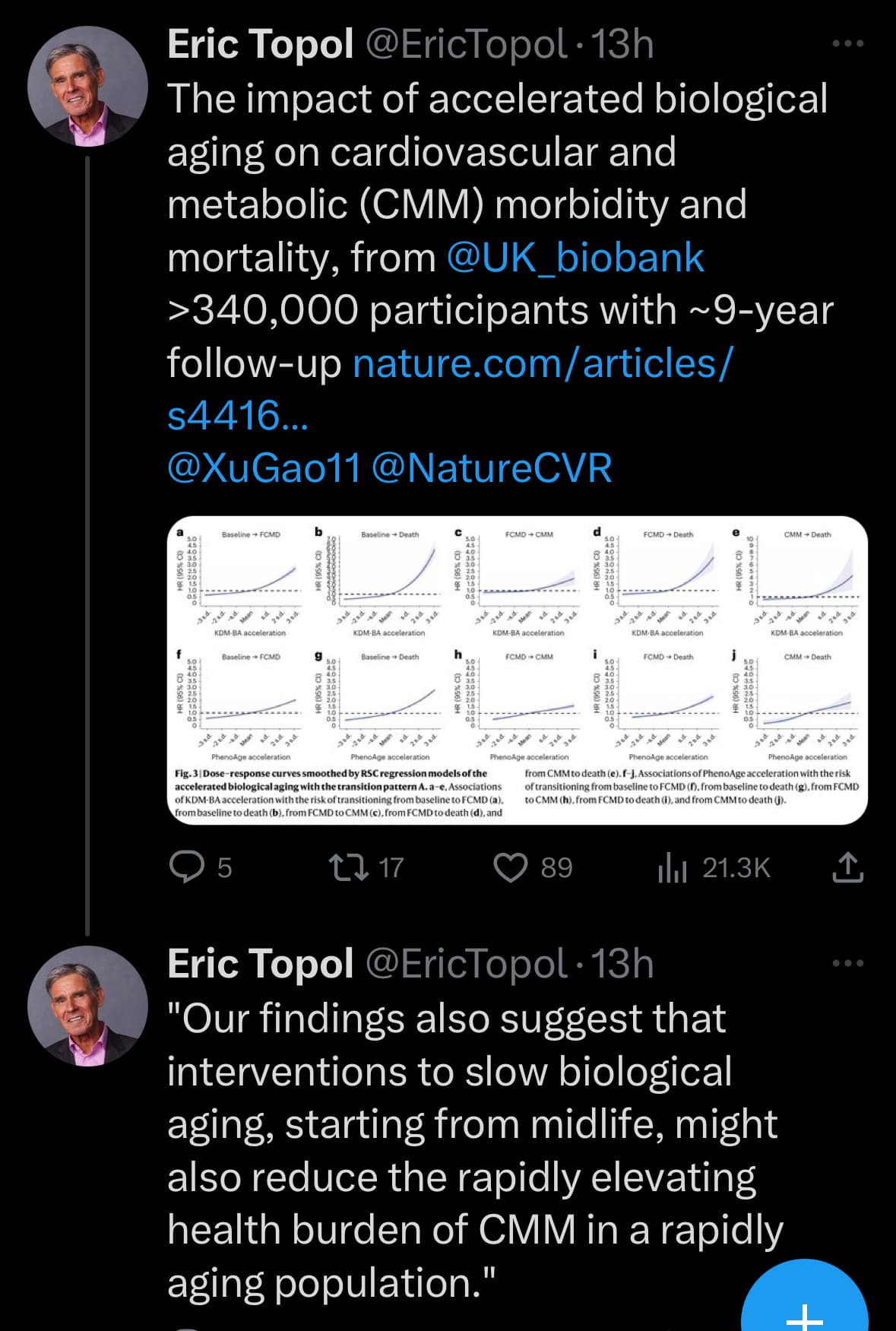
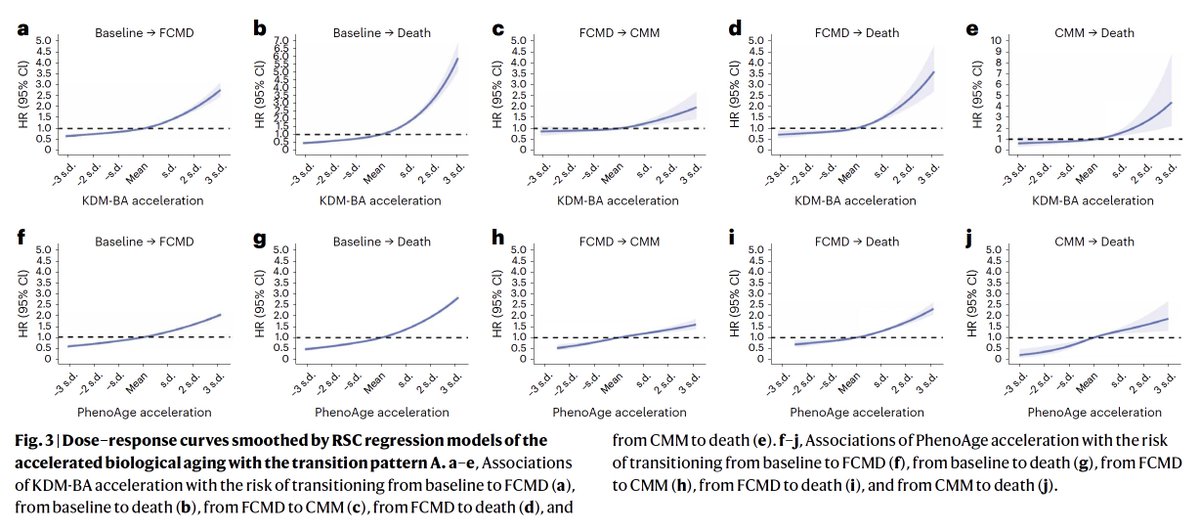
Does this suggest that CVD is a disease of ageing and that maybe it’s not about ApoB levels per se but early intervention to slow down the ageing and restore some functions (reverse cholesterol transport?)?
4 Likes
I don’t think there is any doubt that CVD is a disease of aging, but it also appears to be exacerbated by high levels of ApoB.
4 Likes
I believe that CVD has two important variables that affect it - ApoB and inflammation. Both increase as you age. Both are also alleviated by Bempedoic Acid and Ezetemibe. Rapamycin also reduces inflammation.
Of course this is just a simplified version as there are many other factors involved but I believe these two are the biggest for CVD.
5 Likes
adssx
#308
Inflammation as measured by which marker(s)? And how does bempedoic acid/ezetimibe compare to statins on this?
2 Likes
Inflammation as measured by hsCRP. The literature says BA reduces hsCRP by 20%. For my father, it was reduced by 66%.
4 Likes
adssx
#310
6 Likes