OR
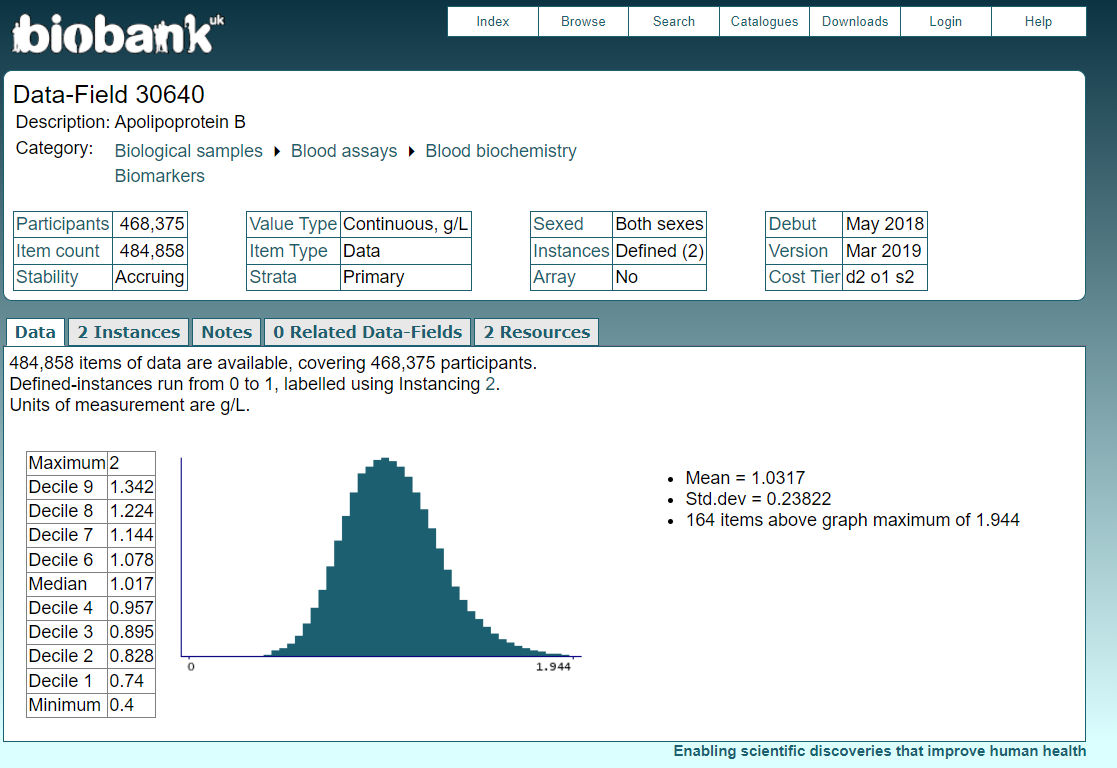
2.) Health influencers, clickbait, snake oil salesmen, random folks with no cardiovascular training or experience, and paper mills saying high LDL is good.
A comment a bit too derisive of the opposing view. The greats were never derisive of each other. (Thinking of the Einstein- Niels Bohr debate. Justice Antonin Scalia and Justice Ruth Bader Ginsburg were good friends. Their families even took vacations together.) But debates nowadays are too strident.
The studies Vlasko and others posted are from scientists, not influencers. But since you prefer youtube videos, here are some “influencers” who are also MDs.
Below is an org that is made up of MDs and scientists.
Among the members are:
Davies, Hywel; MA, DM (Oxon), FRCP (Lond), FACP, FACC. Previously Assoc. Professor, University of Colorado; Chief of Cardiology, Denver VA Hospital; Senior Lecturer and Hon. Consultant physician at Guy’s Hospital, London, UK. Present address: Rue de Condémines 9, CH-1950 Sion, Switzerland.
Kjellevand, Tor Ole; MD, Consultant, Department of Cardiology, Rikshospitalet, University Hospital. 0027 Oslo, Norway.
Mascitelli, Luca; MD, specialist in Cardiology and Sports Medicine; Lieutenant Colonel, Chief of Sanitary Service, Comando Brigata alpina “Julia”, Italian Army, 8 Via S. Agostino, Udine 33100, Italy.
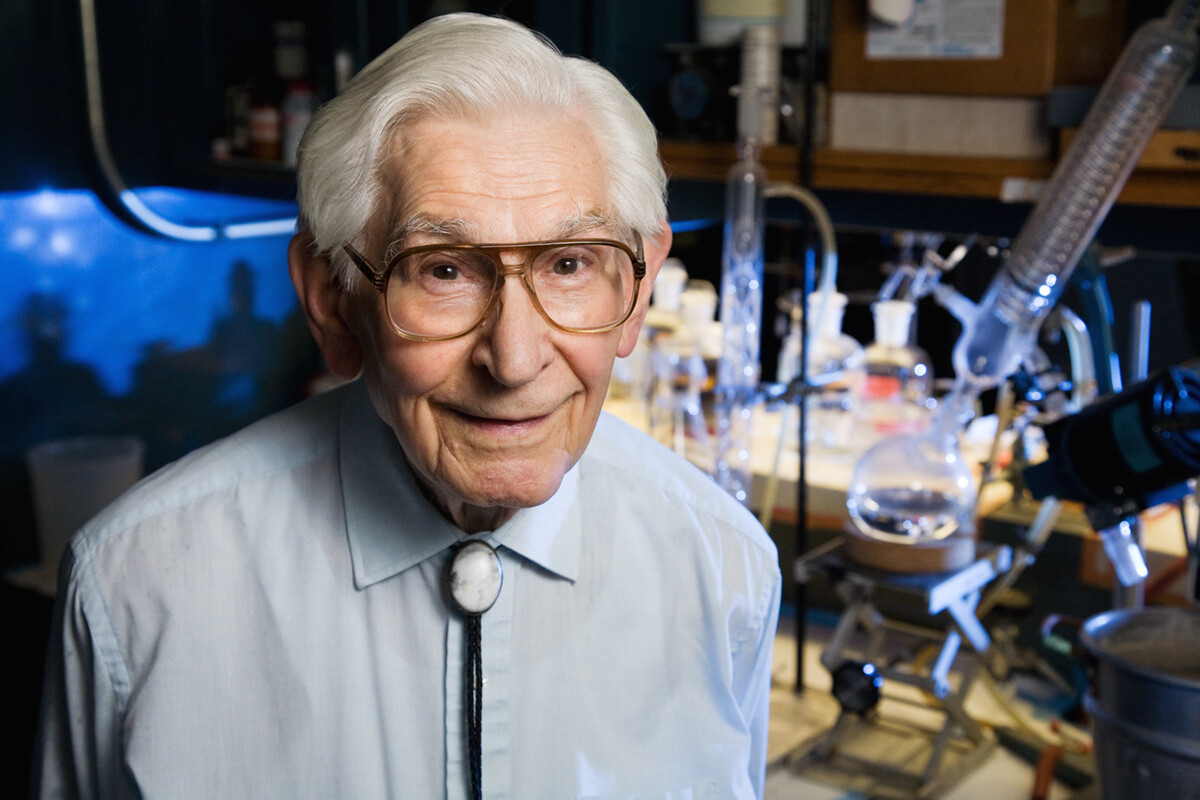
and the late great Fred Kummerow.
Throughout his career, which began in the 1940s, Kummerow challenged orthodoxy in science. His dogged determination to bring to light findings that contradicted popular notions about diet and health sometimes cost him friends and research funds. He argued, for example, that dietary sources of cholesterol like meat and eggs had no influence on heart disease unless they were prepared in a manner that oxidized the cholesterol.
Kummerow’s early work on heart disease led him to realize, decades before anyone else, that artificial trans fats in food were clogging arteries and interfering with blood flow dynamics. His earliest research on trans fats dates to 1957.
Kummerow’s efforts to remove trans fats from foods began in 1968, when he urged the American Heart Association to ask the Institute of Shortening and Edible Oils to have its members reduce the amount of trans fatty acids in shortenings and margarines, replacing them with essential fatty acids such as linoleic acid. The industry reluctantly agreed. That change coincided with a steady decrease in coronary heart disease mortality after 1968, a decline Kummerow saw as additional evidence that trans fats endanger the heart. (Heart disease rates had been climbing before that.)
In 2009, when he was 94, Kummerow filed a citizen’s petition with the U.S. Food and Drug Administration requesting that it “ban partially hydrogenated fat from the American diet.” His 3,000-word petition documented the science linking trans fats in food to inflammation, an increase of LDL cholesterol, a buildup of plaque and an increased risk of blood clots in the coronary arteries.
“Everybody should read my petition because it will scare the hell out of them,” he said at the time.
When the FDA failed to respond to his petition for four years – the law requires a response within 180 days – Kummerow, then 98, filed a lawsuit to force the agency to make a determination on his petition. Three months later, the FDA announced a “tentative determination” that trans fatty acids “are not generally recognized as safe for any use in food.”