mccoy
#1
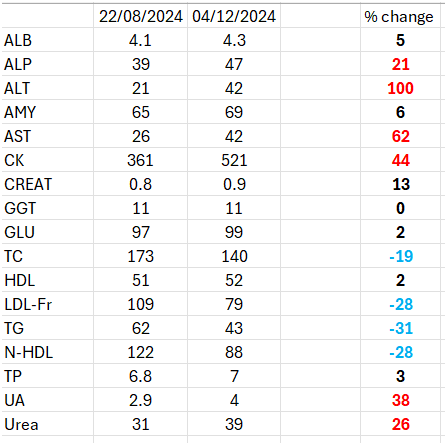
This is my report after I experimented a CVD optimization scheme. After having read various posts in the forum, I tried minidoses of crestor+ezetimibe. 1.25 mg each per day. The purpose was to lower blood lipids without collateral effects. The first part was successful, reduction in LDL, non.HDL and TRIGS of about 30%. The second part was a failure, since the epatic enzymes all increased significantly, even by 100% (doubled their concentration). creatine Kinase also increased. Below, I’m attaching the results of two analyses carried out on capillary blood with the same analytical machinery, before and after, at 4 months of distance. This is clearly not an optimization since liver functions are being apparently detrimentally affected by even very small doses of these drugs. Actually, it’s not clear if it is rosuvastatin, ezetimibe or the combination. Confounding factors? I cannot think about any, barred the introduction of berberine and an increase of 10-20% in saturated fats intake.
6 Likes
A_User
#2
Peter Attia mentions the combination of statins + ezetimibe here and increase in transaminases:
4 Likes
A_User
#3
If you mean in percentage points: I have heard Thomas Dayspring mention that the liver might down-regulate LDL receptors on it to protect itself in case of higher saturated fat intake which is why it would increase serum LDL and apoB. So maybe in combination of up-regulating LDL receptors and a higher SFA intake might not be good, or it’s just as simply as Peter Attia says, inflammation from metabolism from the statins or in combination with ezetimibe. It is probably that as other drugs don’t have the same effect.
I would cease using that combination and try something else personally.
mccoy
#4
I’ve already ceased but now am undecided whether to keep the ezetimibe.
My wife had the same side effect, elevation of hepatic enzymes, with 5 mg crestor alone. The values then decreased switching from crestor to zetia (in parallel with increased lipid values).
In my case, it’s surprising that the elevation of hepatic enzymes took place even in the presence of 1/4 minimum dose of rosuvastatin and 1/8 minimum dose of ezetimibe. I was hoping that the mini doses could avoid this.
In addition, an increase of about 40% uric acid isn’t good news either (OAT2 inhibition?).
1 Like
Davin8r
#5
I’d be suspicious of the berberine, either alone or in combo with the others, as the cause.
3 Likes
mccoy
#6
That’s another thing that I’ll have to evaluate whether to keep or not. At 500 mg/d there are no more big effects on appetite, but other interactions, they would be possible.
1 Like
A_User
#7
I’m trying ezetimibe 10 mg now. I don’t see the reason to keep the dose low, any benefit is welcome and it has almost no side effects.
Berberine is a bit of a weird and dirty drug. Because it has so many effects and somewhat effective for those effects, I’d be vary of it too.
4 Likes
KarlT
#8
I would retest after stopping Berberine. Your LFT’s certainly went up, but not to concerning levels.
1 Like
Pender
#9
I recently tried:
10mg rosuvastatin daily
10mg ezetimibe
My LDL went from 160-180 to 49.
Got it to 85-100 on rosuvastatin alone.
Liver metrics crept up a little, but still in the lower part of the band.
Side effects:
Ezetimibe seems to give me acid reflux, but I’m not positive that’s the cause.
4 Likes
mccoy
#10
I agree that the LFT’s are not very concerning, but the outcome failed an optimization scheme, since I started from about the 40th percentile of atherosclerotic risk (using Non-HDL-C as a proxy). Had I started from the high percentiles the optimization would have been acceptable.
First thing I’ve ceased rosuvastatin, I’m undecided about ezetimibe and yes, I’ll have to think about berberine as well, although it is useful as a mild controller of fasting BG.
Last but not least, I’m going to decrease saturated fats, although this will necessitate increase of some other source of fats or an increase in carbs to avoid catabolism (but then BG homeostasis might need another optimization scheme).
Life was’n meant to be easy!
3 Likes
Just keep in mind that transaminases can come from muscles, not always from the liver.
Peter Attia talked about it on a podcast and said that those increases are usually benign and insignificant, like high creatinine when muscular and supplementing creatine.
The biomarker can become obsolete
3 Likes
Ive had an increase in GERd that lines up with adding ezetimibe, but I’m not sure either
2 Likes
mccoy
#13
But, how can we know that the muscles and not the liver are involved? I’ll have to listen to that podcast (posted by AnUser I think) again, he calls the increase ‘irrelevant’ but on the other side, he says he discontinues the treatment when that happens.
A_User
#14
I haven’t heard about transaminases increasing double from exercise. CK can increase a bit. I think it’s very likely to do with rosuvastatin (and with ezetimibe).
JKPrime
#15
Great presentation. Could you drop everything else including berberine but a statin and repeat the test?
mccoy
#16
Yes, but conceptually I think Rosuvastatin is more likely to have been the culprit in increasing hepatic enzymes; its dose was 1.25 mg/d, that is 1/4 the minimum commercial dose (5 mg) whereas with ezetimibe I used a dosage which was 1.25 mg/d, that is 1/8 the minimum commercial dose (10 mg). Also, my wife experienced a similar increase in hepatic enzymes with rosuvastatin only (5 mg/d, full minimum dosage). Of course, we don’t share a genome except the genes related to ethnicity, but this fact makes me think, also she switched to ezetimibe and the enzymes went back down.
Since I have no difficulties in measuring these enzymes every 3 months, I think I’m going to exclude the statin first, along with berberine, leaving 1/4 or 1/2 the minimum commercial dose of ezetimibe for now.
3 Likes
I don’t have the same issues with ALT and CK, but I do take berberine.
I find with weekly blood tests that there are variations in these things, but I accept that ALT doubling is a thing. CK is quite high as well.
1 Like
Kelsey
#18
Adding bempedoic acid (Nexlizet) really made the difference for me.
1 Like
sudiki
#19
It may be something else (berberine). also, those liver increase results are still w/i normal ranges. I have been taking rosuvastatin and ezetimibe 10 mg each for decades and my annual reports show my ranges about the same or lower in the liver function results and they don’t vary much at all yr to yr. Could also be your body just doesn’t like them…


