I’m not surprised that a plant-based diet low in (saturated) fat and high in fiber alongside exercise helps with various conditions.
3 Likes
A_User
#67
That’s the minimum found in the literature which they used to try and prove statins could clinically significantly regress plaque, basically they had an incentive to find the lowest requirement. Other definitions require more. Since statins doesn’t clinically significantly regress plaque, it cannot nor has not been advertised as such.
The regression in the Ornish study in percent diameter stenosis was 1.75% at the 1 year mark and 3.07% at the five year mark.
The definition of clinical significant regression includes a 0.2 mm or greater increase in minimum diameter as well.
It was 0.01 at the 1 year mark, so it would require a 20 x increase, and at the 5 year mark 0.001, a 200 x increase would be required to meet the criteria.
1 Like
The best bit was when he shit all over resveratrol
1 Like
A_User
#69
Oldest/most papers on heart disease where actual reversal of plaque/stenosis demonstrated
No as there was no reversal of plaque demonstrated, a mere decrease in percent diameter stenosis does not mean so. There needs to be an increase in minimum diameter as well.
Neo
#70
Do you think this is meaningful or meaningless? Or do you think the results are not real?
1 Like
A_User
#71
The result in the graph is meaningless without minimum diameter as I said. If you increase the reference diameter without changing the minimum diameter then the percent stenosis decreases without any regression in plaque. That’s why you need both and it needed to be 200 times larger than it was, and with 7% more reduction in diameter stenosis.
A_User
#73
The point is that the Ornish study or any other study for any other therapy has not shown any regression or reversal of plaque to a clinically relevant degree, and the Ornish study didn’t even show any regression.
The two important points is that the protocol reduced events and plaque didn’t progress.
2 Likes
Ok, I thought you were trying to say that the Ornish study showed no regression but that statin and other drug studies have. Clearly multiple different therapies have shown evidence of “regression”, but the term “clinically significant” is a key differentiator and obviously the thing we actually care about.
One assumption, which may or may not be true, is that regression over time for any treatment is linear, when in fact it could accelerate in a non-linear fashion if continued for longer. In which case plain old “regression” in a short period of time could actually be “clinically significant” if extended long enough.
If we looked at (for instance) a high saturated fat diet for a year and saw plaque progression, should it be dismissed as “clinically insignificant” if it didn’t show enough progression in that limited period of time?
A_User
#75
No, but it wasn’t clinically significant either way.
That statin study did show regression in plaque since minimum lumen diameter improved while percent diameter stenosis decreased unlike the Ornish trial, but it was not clinically significant.
The Ornish trial had a 200x requirement for increase in minimum lumen diameter at 5 year mark, while 20x at 1 year I don’t think there is any evidence it is non-linear.
Plaque progression is a different thing.
I should know better than to open my mouth when I’m away on vacation and can’t really dig into this topic of plaque regression. I hope someone is checking Anuser’s work because I don’t have time to!
1 Like
A_User
#77
If you really want to measure this you should probably do a CT angiogram, to see soft plaque as well, if you’re serious about risk and not just playing around.
- This gives a better sense of the luminal narrowing and the presence of soft plaque
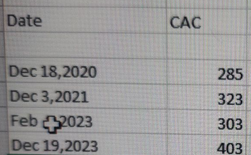
Your CAC has also increased over time…
2 Likes
A_User
#78
50% of fatal MI’s occur in non-calcified areas of coronary arteries.
3 Likes
Where are you getting this “minimum diameter” criterion from? Is it from CCTA, which wasn’t available at the time of the Ornish study?
From where are you getting these numbers?
A_User
#80
It’s in the Ornish study.
Ok, so just to be clear when you say the 0.2mm/10% criteria for “clinically relevant regression in the literature”, you are referring to a single paper when you say “in the literature”, not some firmly-established generally agreed-upon criteria established in cardiology.
Because one could argue that a smaller degree of regression IS clinically significant, based on the positive clinical outcomes in the experimental group of the Ornish study.
2 Likes
BTW, great review paper from 2022 on coronary artery atherosclerosis regression, one of the only ones I could find, published in JACC:
https://www.jacc.org/doi/10.1016/j.jacc.2021.10.035
They use the term “regression” freely for quite a few statin drug studies and note that it isn’t yet known what exactly is “clinically significant”. In fact, “regression” can mean change in plaque quality (from unstable to more stable) without a decrease in plaque volume.
3 Likes
A_User
#83
It’s not one paper and I think that’s how it works.
No, since you are not using what is considered clinically significant reduction in the literature. Either way, in that case you would have to accept that a progression of disease is clinically significant reversal of ASCAD because it also can coincide with a reduction of outcomes. It makes no sense. It is not reversal of plaque and thus atherosclerotic coronary artery disease (ASCAD).
If you see my responses to @Neo you will see why you need an increase in minimum diameter as well and why it is included in the definition.
I’d recommend reading the review paper I posted. The cut-off point for “clinically significant” is subjective/unknown when applied to diameter stenosis and MLD based on the current state of the literature. Smaller changes can be clinically (i.e. real-world) significant, as suggested by outcomes in the Ornish study.
A_User
#85
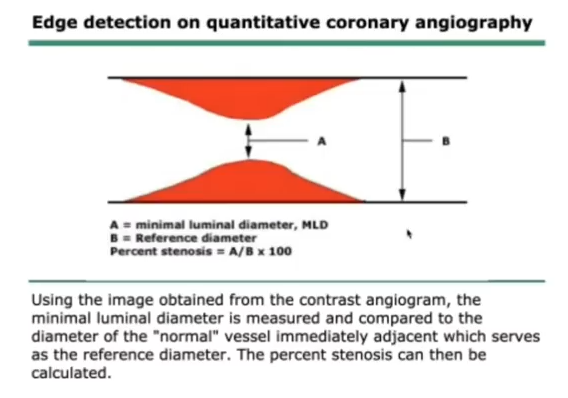
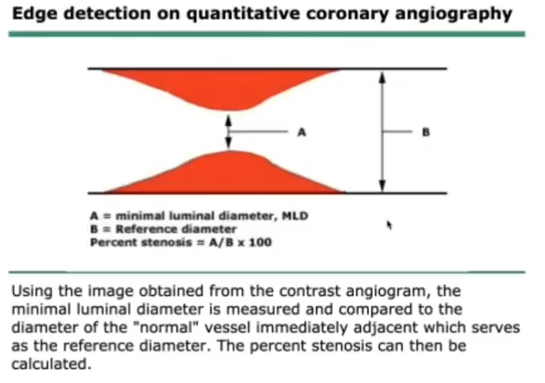
It’s not unknown and all definitions are subjective, unless you want me to argue for definitions being objective, and the Ornish study used Quantitative Coronary Angiography, so you need a definition for clinically relevant regression (or regression at all) pertaining to that.
Or rather an intervention can improve outcomes without regression of plaque, clinically relevant or not… There was no regression as a result of the intervention.
Read again why minimum lumen diameter has to increase.
If you accept that reversal is a decrease in percent stenosis without an increase in MLD (which can happen because the reference diameter increases, like vasodilation), then you’d have to accept that pomegranate juice reverses disease, which Ornish has studied, or nitrates, and a bunch of other interventions with similar results.




")