adssx
#62
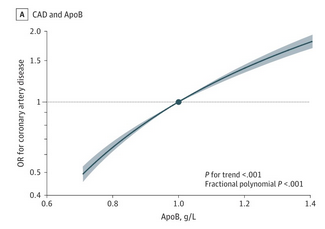
They wrote “no threshold” but the image stops at 0.7 g/L? Do they have data below that? If so, why didn’t they plot it? If not, why did they write “no threshold”?
1 Like
I don’t see how a 200 year old person could develop ASCVD with an LDL-C of 40mg/dL or lower.
1 Like
Won’t LDL deposit irreversibly on the walls of arteries, so if LDL levels are high enough to see a non-zero deposition rate, eventually deposits will build, albeit more slowly with lower LDL levels. Do i understand this correctly?
We have studies that indicate that plaque buildups can reverse to some extent as levels as high as 80mg/dL. The body apparently has the ability to remove deposits from blood vessel walls to some extent.
The effects of lipid-lowering therapy on coronary plaque regression: a systematic review and meta-analysis | Scientific Reports (nature.com)
2 Likes
A_User
#66
See previous discussion here too:
2 Likes
I’m listening to a podcast with Thomas Dayspring and he just said we can have a zero blood TC and this should be fine. Seems different to what others have said or the j/u shaped curve.
A_User
#68
There is no evidence of a U-shaped or non-linear curve. See the genetic evidence, totally linear, just like in the RCT’s.
I have also heard Peter Attia say serum LDL / ApoB is just useless and that ApoA1 / HDL can take over the functions of it. It is probably trash from evolutionary past useful in case of famine (antagonistic pleiotropy). Evolution only cared about humans reaching reproduction age and a bit longer.
I’ve heard that all the cells in the body can produce their own cholesterol.
I haven’t paid so much attention to these arguments as they are not so important.
1 Like
JuanDaw
#69
I meant low TC was the worst performer within each age group. That is why I said read horizontally.
scta123
#70
You shared this article:
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.116.023359
Let me use your argumentation. There was a 100% increase in fatal MI in rosvustatin group vs. placebo.
A_User
#71
Where it says…
Cardiovascular therapeutics should aim to reduce mortality, but it is not necessary to demonstrate a reduction in all-cause mortality when assessing them. It is, in general, misguided to attempt to demonstrate such an effect because it is too crude a measure of either benefit or harm.
Specifying the primary end point to be cause-specific mortality rather than all-cause mortality does not mean that serious adverse events because of an intervention are ignored. These events are recorded and, if there is a significant excess of a particular cause of death, that is taken into account when considering the overall balance of harms and benefits of the intervention.
That’s not how this works. You can’t just take a number out of a combined endpoint, and use it with no p-value.
1 Like
adssx
#72
Yes this confirms that they have no data below 0.7 g/L but actually they wrote “suggesting no threshold” so they carefully chose their words and indeed the curve suggests a lack of threshold (at least until 0.7 g/L).
2 Likes
I believe understood your instructions. But if we’re not pre-briefed to ignore age, any statistician would immediately see the far stronger relationship in that table between age and ASCVD. I am only asking is there something we can change to mimic a younger age for ASCVD that could be a stronger impact than lowering LDL (which has been shown to be causal)? It wasnt trying to be a baiting or “gotcha” question: we are largely here on this forum trying to lengthen our lifespan or even “de-age” ourselves. Maybe there is a characteristic (such as inflammation — just an example) that could have a major impact.
(Virtually every professional research scientist i know skips all the text in every single research note they read and immediately go to the figures)
1 Like
9 vs 6 is only 50% increase and overall there are 31 vs 37 deaths (according to your definition) so rosuvastatin reduced deaths from any cardiovascular disease by over 17%.
scta123
#75
I just wanted to demonstrate how stupid is using relative numbers… but anyway.
If you still think that JUPITER is the gold standard of statin use in primary prevention and as @A_User said, a wonder drug, sure, knock yourself out.
I do believe that statins are wonder drugs that can and will massively extend median lifespan in genetically diverse humans, especially if started early enough.
1 Like
JuanDaw
#77
Agreed we are all here to look for ways to extend our stay on this earth. I did not imply any gotcha from your observation. My apologies if that is what came across.
But this being a cholesterol thread, I focused on what jumps out from the figures - that low TC is bad for CVD and all cause mortality, for all age groups, within that study population. Now can we improve on reduction of CVD risk by other means? Agreed we can. That, I believe, is being discussed in other threads.
3 Likes
No apologies are needed but thanks anyway. I just wanted you to know i was merely asking for my own knowledge, not “defending a tribe” or belief. I’m here to learn. I appreciate your thoughts.
3 Likes
JuanDaw
#79
The French paradox as exemplified by stats between Belfast and Toulouse.
https://vernerwheelock.com/40-heart-disease-belfast-or-toulouse/
Northern Ireland has one of the highest death rates due to heart disease in the world while France has one of the lowest. A comparison between the diets of middle-aged men in Belfast and in Toulouse which was published as long ago as 1995 provides some fascinating insights which are highly relevant to anyone interested in understanding how diet and health/disease are related (1).
TABLE 1 DEATH RATES IN BELFAST AND TOULOUSE
| Death rates/100,000 |
|
|
|
|
|
Men aged 45-54 |
|
Men aged 55-64 |
|
| Cause of death |
Belfast |
Toulouse |
Belfast |
Toulouse |
| Ischaemic heart |
237 |
56 |
761 |
175 |
| Stroke |
32 |
24 |
130 |
61 |
| Other CVD |
30 |
22 |
130 |
92 |
| Cancer |
188 |
159 |
694 |
515 |
| Injury and poison |
59 |
75 |
67 |
72 |
| Other |
91 |
122 |
330 |
280 |
| All causes |
638 |
459 |
2112 |
1197 |
TABLE 2 RISK FACTORS FOT HEART DISEASE IN BELFAST AND TOULOUSE
|
Men aged 45-54 |
|
Men aged 55-64 |
|
| Risk factor |
Belfast |
Toulouse |
Belfast |
Toulouse |
| Diabetes(%) |
2.6 |
7.2 |
3.5 |
10.9 |
| Hypertension(%) |
20.6 |
27.5 |
33.5 |
49 |
| Cigarette smoker(%) |
32.3 |
35.3 |
22.9 |
36.2 |
| TC(mmol/L) |
6.19 |
5.94 |
6.12 |
5.98 |
| HDL cholesterol(mmol/L) |
1.22 |
1.39 |
1.28 |
1.34 |
| BMI |
26.3 |
26 |
26.7 |
26.4 |
Belfast TC is 236 (6.12) versus 231 (5.98), so almost equal. BMIs are almost equal.
The French are more diabetic, more hypertensive, and smoke more. But the French die less. Hard to believe that HDL explains it all.
2 Likes
medaura
#80
I’ve got no dog in this fight and am genuinely agnostic, while reluctantly accepting the consensus for now when it comes to what to aim for (i.e., low is good).
Only chiming in to say that the way @Virilius and @A_User conduct their advocacy for their position is extremely off putting to someone on the sidelines and I have to actively remind myself that even sound causes have obnoxious proponents, so as to not let my judgement be clouded. At the margins though you’ll convince more people if you insult less—make of that what you will unless your purpose isn’t really to change minds but rather satisfy your own aggression in these forums.
About the issue at stake, I repeat I’m genuinely agnostic but my uninformed intuition is that there’s likely some sort of catch-22 effect at play, not only with cholesterol / apob but with most key markers of health and longevity, meaning mother nature wants us off the stage around our expiry date and has multiple redundant traps prepared so route to death can be a bit of “choose your own adventure.” Cholesterol very probably is atherosclerotic so its cumulative circulation above a certain threshold will increase odds of plaque and its thickness over time. But it also seems to play important roles in the immune system in part to keep microbial burden in check, so its removal could lead to excess accumulation of inflammation which will leave the body vulnerable to some other mode of death, possibly cancer. Yes heart disease is the #1 killer but I’m not convinced apob/ldl manipulation won’t just lead to an overall musical-chairs dynamic with death’s top hits. Perhaps it will add a few years of life on average before the next source of death strikes. Perhaps…. But how many years of life will some people waste debating it on forums like this?
There are a few master levers of longevity out there, mTOR seemingly one, that will genuinely stretch out our expiry date systems-wide. I hope more are discovered and deployed. Personally I don’t believe ldl will move the needle all that much at the end of the day. And whoever neglects his health’s fundamentals like sleep and nutrition thinking he’s covered because he’s been taking a statin since his 20s is deeply deluded and will find out one day.
Two cents tossed in the ring. Peace out 
11 Likes
AnUser and I are both in our 20s. Maybe our assertive style of arguing is an indicator of youthfulness?
4 Likes