yes. had my first lipid tests two years ago and turned out i had familial hypercholesterolemia. My apoB was 175 mg/dl. after 20 mg rosuvastatin it went down to 87 mg/dl. I told my Doctor that i wanted to try adding ezetimibe 10mg. After adding that my apoB is now around 30 mg /dl. My grandfathers had heart issues and with my genetically high lipids it was easy for me to convince my doctor that i wanted to be aggressive in preventing ASCVD.
1 Like
One of my male colleagues had a stroke last week at work. He’s still in the hospital. He had high blood pressure and cholesterol. He is in his mid-50s, thin as a rail, and goes hiking on the weekends. He knew about his problem but tried to address it with diet and exercise.
Sometimes you just need a statin and telmisartan. I hope he makes a full recovery, but we don’t know how bad it is.
6 Likes
scta123
#108
A friend of mine also suffered transient ischemic attack (TIA) a week ago during lunch we had together. He is also very sporty but ignores his high BP and high cholesterol. He is also in his mid fifties. It was quite scary. I hope he will address is seriously. If you watch The Crown on Netflix, episode on Margaret shows very realistically how a decline following a TIA can be quite drastic and fast.
With one word, prevention!
4 Likes
It turns out it wasn’t a bad stroke. He’ll be back to work after taking a month off to recover. I hope he takes it seriously from now on. It’s a wake up call.
4 Likes
A_User
#111
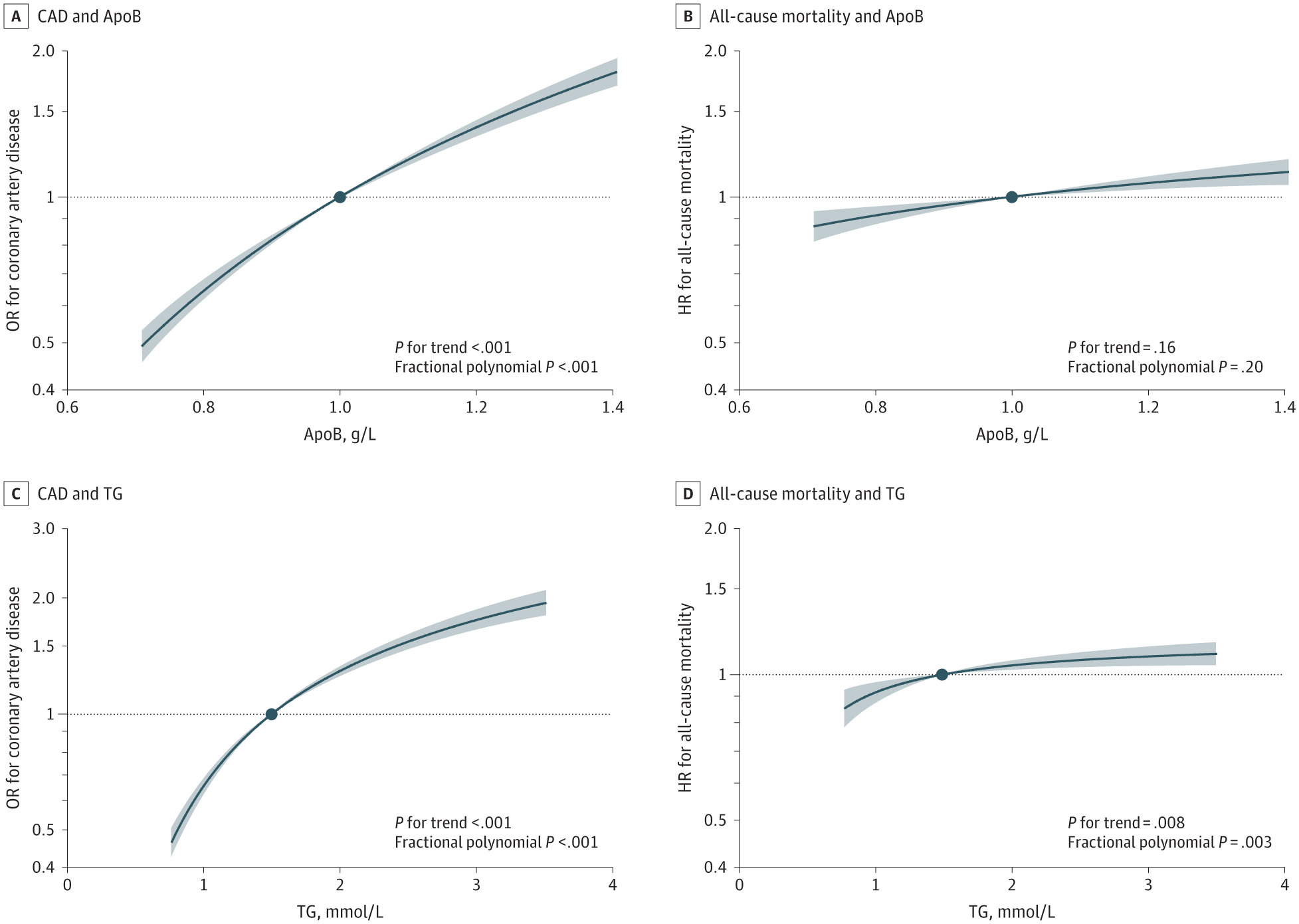
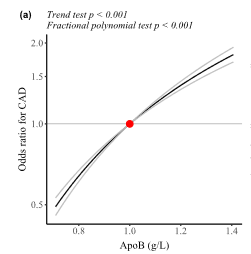
Consistent with RCTs7,8,15,16 and previous MR studies,3,5,23,24 in this genetic association study, we found positive associations of genetically predicted apoB and LDL-C with CAD, all-cause mortality, and CVD mortality, and genetically predicted TG was positively associated with CAD. Our investigation has added to the evidence base by showing such associations hold across the whole distribution of apoB, LDL-C, or TG.
Our findings provide genetic evidence suggesting no threshold of lowering apoB or, equivalently, LDL-C (ie, the main apoB-containing lipoprotein) for reducing risk of CAD, all-cause mortality, and CVD mortality, further supporting the concept of the lower the better. The retention of apoB-containing lipoproteins in the artery wall and subsequent release of cholesterol contents are essential for the initiation and progression of atherosclerosis.46 Our findings are consistent with RCTs8-10 showing that intensive LDL-C lowering further reduces CVD events compared with standard LDL-C lowering. However, most RCTs9-13 failed to show significant incremental benefits of intensive LDL-C lowering on all-cause mortality or CVD mortality. This discrepancy may be related to insufficient difference in LDL-C between groups, short follow-up duration, and low proportion of death from CVD in RCTs,9-13 or differing effects on mortality between LDL-C lowering therapies.47 Notably, a trial48 has shown high-dose statin therapy further reduces all-cause mortality compared with low-dose therapy in Japanese patients with the mean LDL-C less than 90 mg/dL (to convert to mmol/L, multiply by 0.0259) at baseline. Our findings are consistent with a recent MR study49 showing no threshold in the association of LDL-C with CAD, although that study used a different approach for instrument selection and lacked power to detect a significant association of LDL-C with all-cause mortality.
Of course even low apoB had high odds ratio from increasing apoB, hence lower is better. See the explanation below why higher stratums had a decreasing odds ratio for increases in apoB although still positive.
The decreasing association of genetically predicted LDL-C with CAD risk as LDL-C increases should be interpreted cautiously because fewer individuals with higher LDL-C survived to be recruited50 and more of them died during follow-up,51 which may lead to an artifact of less harmful effects. Prevalent statin use could mitigate the genetic association of LDL-C with CAD risk, particularly in people with higher LDL-C.52 It is also possible that the decreasing association reflects effect heterogeneity in population groups with different demographic characteristics rather than nonlinearity for any specific individual. Furthermore, LDL-C confers greater absolute risk of CAD in people with higher LDL-C than people with lower LDL-C, even for the same relative risk.
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2814089
1 Like
L_H
#113
The observed distribution in the study only goes as low as 71mg/dl. How do you know the lowest level is too high?
A_User
#114
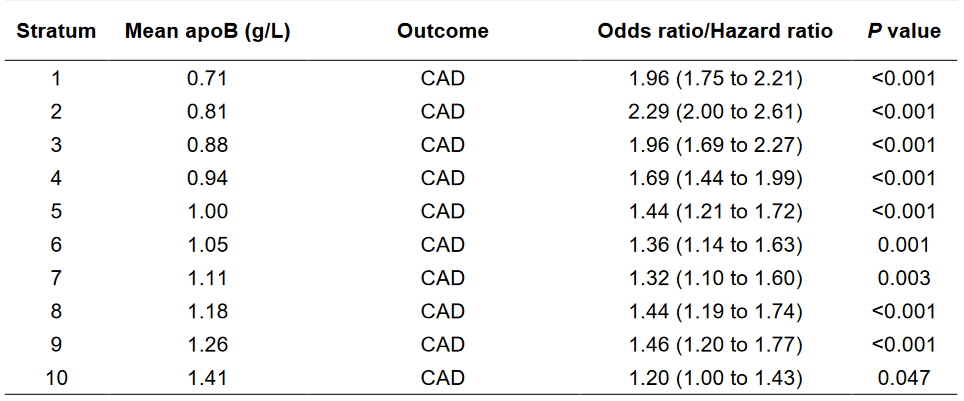
See the odds ratio for stratum 1 with the nonlinear MR.

L_H
#115
What are you trying to say?
A_User
#117
@L_H @scta123 it seems I misunderstood the stratums, the odds ratio / hazard ratio is per 1 SD increase from the mean in the stratum. So an increase from 71 mg/dl to 95 mg/dl has a 1.96 increase in odds ratio for CAD, for instance. But it shows 95 mg/dl is very bad compared to 71 mg/dl, nearly twice the risk!
It’s easy to assume that even lower will be better, maybe twice as good…
1 Like
L_H
#118
Yes, unfortunately it doesn’t tell us anything about apo b lower than 70.
The all cause mortality curve is flatter than I would expect from the CAD curve alone.
1 Like
Anyone having negative side effects from using PCSK9i?
Davin8r
#121
Other than the 10 seconds of stinging during the injection, none whatsoever. I’ve been on Repatha or Praluent for several years (had to switch at one point per insurance requirement). I can’t tolerate any dose of any statin without muscle/joint pain.
2 Likes
Neo
#122
Nothing I’ve noticed or seen in any blood work.
2 Likes
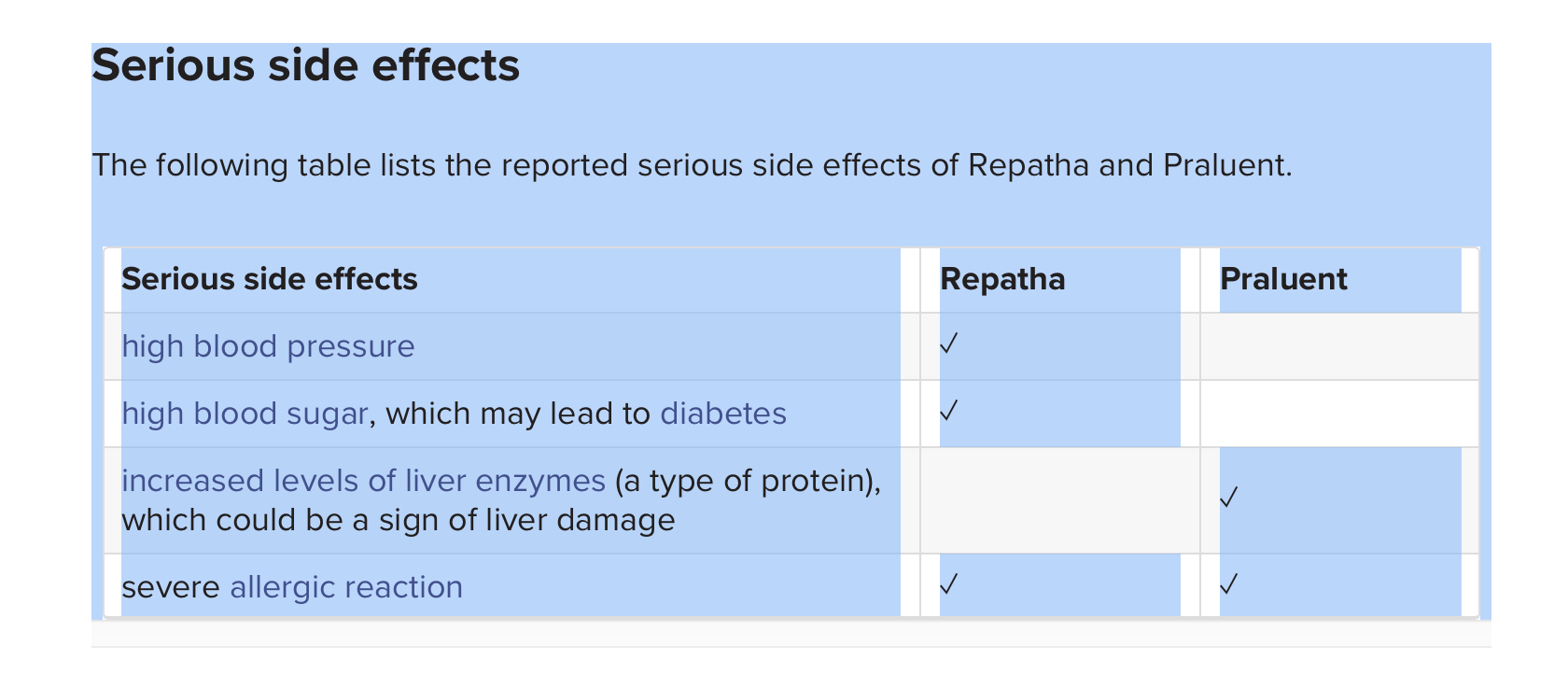
see this chart I found online at medicalnewstoday.com. I’m concerned about the blood pressure and glucose potential side effects for Repatha as well as the liver issue with Praluent. For those on either of these meds, do you share those concerns?
1 Like
Neo
#124
I’m not able to see the chart/correct sorry, just their main home page when I click on the link
I take Repatha and have personally not seen any issues on the things you pasted, but that is only an N=1
Suggest
- look at the trials for data
- most importantly, those things are easily measurable, so measure and look at those biomakers more frequently in the beginning to see how your N=1 biology works either the PCSK9i
2 Likes
It’s best to monitor these factors. It won’t affect everyone as we all have distinct biologies. Just be aware that they could happen and be on the lookout for these side-effects.
1 Like
Is anyone aware of studies on the marginal benefits of aggressively lowering metrics such as apo(b) and LDL-C with drugs such as Bempedoic Acid after reaching the 70’s and 80’s? My sense of the larger picture is that there are lifelong benefits to keeping baseline inflammation metrics low, and maintain generally healthy blood metrics – same for blood pressure and other health indices – but would we expect to see incremental benefits for an 80 year old reducing apo(b) from, say, 100 to 50?
3 Likes
A_User
#127
Longevity syndromes: Familial hypobeta and familial hyperalpha lipoproteinemia (1976)
Longevity and morbidity and death from myocardial infarction were examined in eight kindreds with familial hypobeta lipoproteinemia and in 18 kindreds with familial hyperalpha lipoproteinemia. Expectation of life for males and females from kindreds with hypobeta lipoproteinemia was 9 and 12 years longer (p ≤ 0.002) than that indicated by population statistics for U. S. white populations, whereas expectation of life for males and females from kindreds with hyperalpha lipoproteinemia was 5 and 7 years longer (p < 0.02). Morbidity from myocardial infarction in 115 living first-degree adult relatives of probands with hypobeta and hyperalpha lipoproteinemia and in 364 living first-degree adult relatives of normolipemic spouse controls were compared. Nonfatal myocardial infarction (MI) was reported for 18 of 364 (5 per cent) relatives of normal spouse controls and in 0 of 115 relatives of hypobeta and hyperalpha subjects (p < 0.05). The ratios (mean ± S.E.) of C-LDL to C-HDL in familial hypobeta and hyperalpha lipoproteinemia were 0.79 ± 0.06 and 1.21 ± 0.06, as compared to 2.41 ± 0.12 in a control population (p < 0.001). If high-density lipoproteins confer protection against development of atherosclerosis, whereas low-density lipoproteins have opposite effects, then we speculate that the low ratio of C-LDL:C-HDL may be related to prolonged longevity and decreased morbidity from myocardial infarction in familial hypobeta and hyperalpha lipoproteinemia.
https://www.translationalres.com/article/0022-2143(76)90516-3/abstract
1 Like
LukeMV
#128
Well I didn’t check Apo-B this time but my LDL was 32. Lowest I’ve ever had. I’ve been taking 5mg Rosuvastatin and 10mg ezetimibe so I will drop the ezetimibe. My uric acid is too low for my comfort at 3.8 and read they can lower it, so I think dropping the ezetimibe is a good idea.
2 Likes