A_User
#127
Longevity syndromes: Familial hypobeta and familial hyperalpha lipoproteinemia (1976)
Longevity and morbidity and death from myocardial infarction were examined in eight kindreds with familial hypobeta lipoproteinemia and in 18 kindreds with familial hyperalpha lipoproteinemia. Expectation of life for males and females from kindreds with hypobeta lipoproteinemia was 9 and 12 years longer (p ≤ 0.002) than that indicated by population statistics for U. S. white populations, whereas expectation of life for males and females from kindreds with hyperalpha lipoproteinemia was 5 and 7 years longer (p < 0.02). Morbidity from myocardial infarction in 115 living first-degree adult relatives of probands with hypobeta and hyperalpha lipoproteinemia and in 364 living first-degree adult relatives of normolipemic spouse controls were compared. Nonfatal myocardial infarction (MI) was reported for 18 of 364 (5 per cent) relatives of normal spouse controls and in 0 of 115 relatives of hypobeta and hyperalpha subjects (p < 0.05). The ratios (mean ± S.E.) of C-LDL to C-HDL in familial hypobeta and hyperalpha lipoproteinemia were 0.79 ± 0.06 and 1.21 ± 0.06, as compared to 2.41 ± 0.12 in a control population (p < 0.001). If high-density lipoproteins confer protection against development of atherosclerosis, whereas low-density lipoproteins have opposite effects, then we speculate that the low ratio of C-LDL:C-HDL may be related to prolonged longevity and decreased morbidity from myocardial infarction in familial hypobeta and hyperalpha lipoproteinemia.
https://www.translationalres.com/article/0022-2143(76)90516-3/abstract
1 Like
LukeMV
#128
Well I didn’t check Apo-B this time but my LDL was 32. Lowest I’ve ever had. I’ve been taking 5mg Rosuvastatin and 10mg ezetimibe so I will drop the ezetimibe. My uric acid is too low for my comfort at 3.8 and read they can lower it, so I think dropping the ezetimibe is a good idea.
2 Likes
An interesting question is what the concern is about low urate/uric acid. High urate can cause gout, but I don’t know what low urate cases.
1 Like
LukeMV
#130
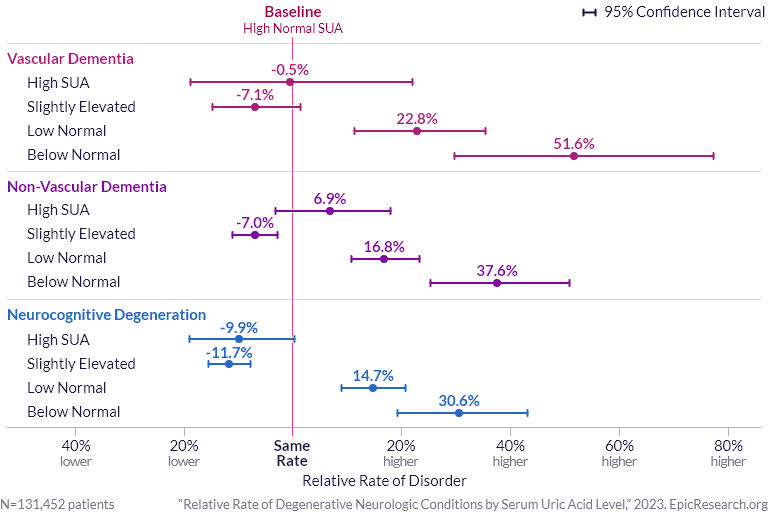
There’s a dementia link with low uric acid (albeit this is at 3.5)
Mike Lustgarden also said in a video that 5.0 seems to be the uric acid level that is optimal for longevity but I don’t remember where he got that number from.
1 Like
Is there any medication which increases/decreases uric acid (as a side effect)? If so, has it affected dementia rates?
A_User
#132
Uric acid seem something like you should be able to find mendelian randomization data for though non-linear (U-shape) curves are usually hard to detect.
LukeMV
#133
There are a few that decrease it. Empagliflozin (or any SGLT2), which I also take, lowers it too, but the benefits of that one far exceed the risks in my case IMO.
I don’t think any are directly linked to dementia though.
3 Likes
A preventive cardiologist pretty much agrees with you
3 Likes
No negatives. Reduced Lp(a) from 40 mg/dl to 29mg/dl and also reduced LDL/C and APOB substantially after 9 months.
Neo
#136
Here are first two hits on google - I have not spent time looking at what is consensus / where there is debate
acid is also an antioxidant and low levels can result in oxidative stress and endothelial dysfunction
Uric acid levels below 3.5 mg/dL are correlated with increased rates of being diagnosed with non-vascular and vascular dementia
1 Like
Neo
#137
food wise I saw this
may want to add more purine-rich foods to your diet, with a focus on healthier options like fish, fruit and full-fat dairy
think good fish and good fruit should be positive re dementia, but would watch the amount of sugar from fruit
After about 8 months on Repatha, no change to blood pressure – it was and remains low-normal. My HiAc is 5.8 – but it has been at that level since 2017 if not earlier. I have been on Metformin. Don’t know how concerned to be about the prediabetes --will be seeing an endocrinologist soon. I have many reasons to believe it is genetic. In any case it doesn’t appear to have gotten worse since starting Repatha.
1 Like
L_H
#139
I really like this article. The next (on nutrition and apob) should be interesting too.
"I feel he strays too far from the science, however, when he advocates for LDL-C goals of <20 mg/dl seemingly for all individuals, irrespective of their overall lifetime risk of cardiovascular disease. Achieving these goals would require multiple different cholesterol-lowering medications.
Recently, Attia revealed that he is taking 3 different cholesterol medications, Bempedoic Acid, ezetimibe and a PCSK9 inhibitor. This is the kind of cocktail that would be needed to get his patients to the goal he recommends.
For many individuals at a low to moderate lifetime risk of ASCVD this makes little sense. There would be very little benefit from reduction of ASCVD risk at a substantial financial cost and at the risk of significant side effects.
Furthermore, Attia is suggesting lifetime treatment for two of the three drugs he takes (and presumably prescribes). We don’t have data beyond 5-10 years on long-term side effects"
1 Like
Considering 1 in 6 people will die from cardiovascular disease, addressing it seems to be of high importance. They say that if we can cure cardiovascular disease, life expectancy will rise by 2.5 years.
So, based on my back of the envelope calculations, those lucky 1 in 6 individuals would gain 15 years of extra lifespan if they could prevent their death from cardiovascular issues.
4 Likes
A_User
#141
Around 1 in 3 die from cardiovascular disease worldwide in 2016, lets not ignore non-fatal heart attacks and strokes either which for example statin treatment prevents (there’s lots of controlled studies, I have posted them elsewhere clearly showing statins causally decrease stroke). Overall having optimal lipids with the help of drugs throughout life, blood pressure, healthy diet high in vegetables and fruits with a low sodium intake is going to have a great effect on both life- and healthspan.
1 Like
LukeMV
#142
The two leading causes of death and how to prevent them
Cardiovascular death prevention = ApoB under 60 and optimal systolic blood pressure of 100-110
Cancer prevention = combined resistance and aerobic training
3 Likes
A_User
#143
There might also be pleiotropic effects from certain treatments like statins which also help the effect outside of lipid lowering.
1 Like
Neo
#144
Think cancer is more tricky than cardiovascular (which itself is a bit more complex than that).
For cancer, I don’t think we are close to being able to fully prevent yet. So a good program also needs a lot of earliest possible detection/screening.
5 Likes
LukeMV
#145
Definitely. Just wanted put in some basic info in there.
1 Like
L_H
#146
I think that’s a good way of looking at it. And even if its 1 in 3 that’s still 7.5 years from avoiding cvd. Plus the quality of life. The “skeptical cardiologist” who wrote the article is a proponent of low apoB, he’s just not targeting extreme (20ng/dl) levels. He’s aiming for 40s plus low inflammation.
2 Likes