scta123
#147
Centenarians have lower levels of uric acid.
A_User
#148
You need to show more evidence than just that to show that low uric acid levels are good.
3 Likes
Been wondering why apoB is a better metric than ldl, or if “lower apoB is better “ all the way down? The simplistic explanations I received for years have left me confused…but no more.
Listen to the magnificent Dr Vyvyane Loh explain what is happening.
3 Likes
Are ApoB and LDL ever uncoupled? That is: Can a person have high LDL and low ApoB or vice versa? My own seems to track; low LDL=Low ApoB. Not a strictly linear function, but generally speaking.
2 Likes
A_User
#151
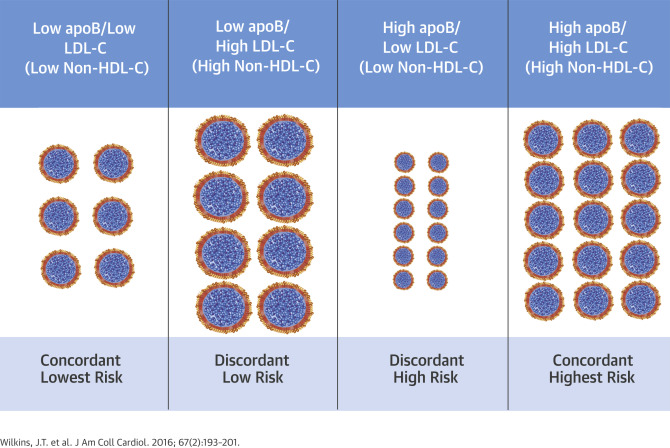
Yes that’s possible and it does happen, it’s called discordance between LDL and apoB.
5 Likes
L_H
#152
Yes, ldl particles come in different sizes. So for example having large ldl particles would mean higher ldl-c ( a volume measure) relative to apob (a number of particles measure).
LukeMV
#153
@A_User @L_H It has to be super rare though, right? I wonder how it could even happen from a lifestyle standpoint. I guess as long as the ApoB low, it’s alright I suppose.
L_H
#154
Yes apob is thought to be “mechanistically” the key indicator, and ldl-c is thought to be merely a proxy indicator for apob. (According to Dayspring/Attia)
It’s not rare for there to be some variance in particle size. Omega 3 and olive oil for example, seem to increase particle volume and so can mean apob is lower relative to ldlc. Veg/seed oils like Canola oil may do the opposite.
Dayspring/attia convincingly argue that the key is to focus on apob rather than ldlc. And there is now plenty of research evidence that it’s a better predictor of cvd.
But there may be better indicators, yet to be developed, which focus on oxidation and apob.
4 Likes
A_User
#155
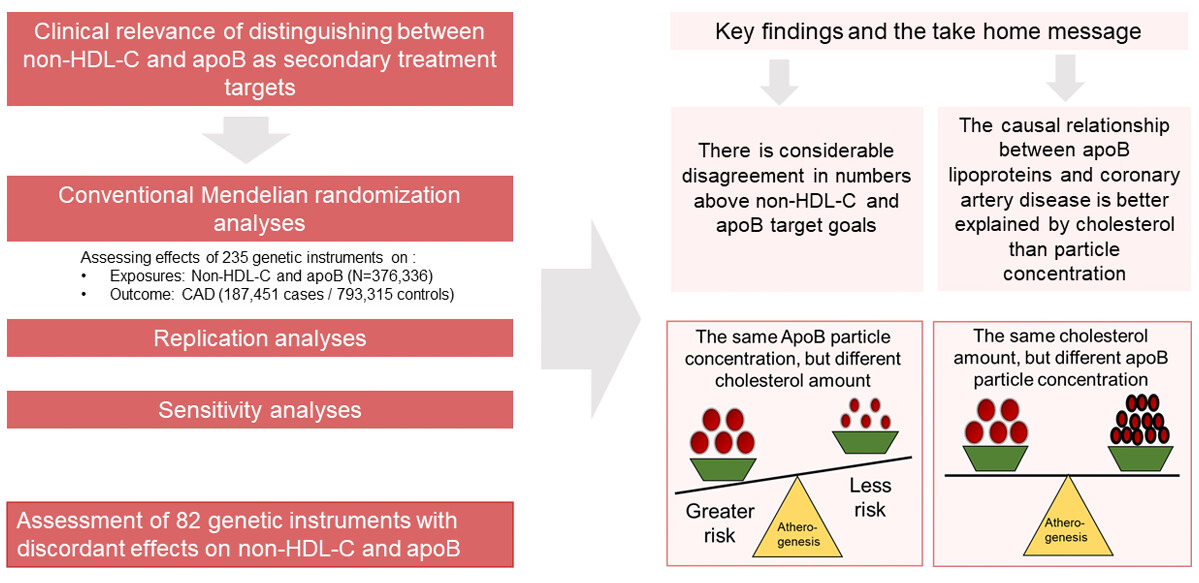
Non-HDL-c is an independent risk factor from apoB according to a MR study I looked at long ago. So risk doesn’t decrease all the way (low apoB and low non-HDL-c is lowest risk).
L_H
#156
Really keen to see the study if possible.
LukeMV
#158
If one goes down, does the other also tend to go down with it? I got my ApoB under 50 but haven’t gotten my Non-HDL checked before. Is there a way to calculate non HDL without getting the direct blood test for it?
A_User
#159
Yes they are highly correlated. Total cholesterol minus HDL cholesterol and you get it. That’s the mass of all apoB particles.
1 Like
ng0rge
#160
@A_User , you should know that this statement is misleading. I just read through the article you took it from and the author is strongly convinced and says that there is plenty of evidence that ApoB is a much better marker. He is arguing against this one study that says otherwise.
" First, Mendelian randomization is a powerful, but not an all-powerful, tool, and the superiority of apoB has been demonstrated by a variety of analytical methods, including Mendelian randomization. Second, if Helgadottir et al. are correct, an individual with a normal LDL-C but a high apoB is not at increased cardiovascular risk, whereas a patient with a high LDL-C but a normal apoB is. But this does not square with the indisputable reality that cholesterol-depleted apoB particles are much more common in patients with arteriosclerotic cardiovascular disease than cholesterol-enriched apoB particles. Moreover, their conclusions stand at variance with many other reports, which also should not be dismissed. Third, apoB is measured more accurately and precisely than LDL-C and non-HDL-C. Therefore, as a practical clinical tool to judge the risk and the adequacy of therapy, apoB is superior to LDL-C and non-HDL-C. The fourth and final point—the point I am most certain of—is that apoB is not all-informative. There must be factors that influence the entry of apoB particles into the wall and there must be factors that influence their binding to the arterial wall."
A_User
#161
How do you determine what is misleading?
Every quote is misleading then.
I posted the link to the article: I am not going to copy paste all the text here.
ng0rge
#162
Hey…calm down. This is not rocket science. You selected 2 sentences to quote out of the whole article. They were misleading and did not represent the article. What I quoted from the article was representative of what it was saying…AND you KNOW that.
A_User
#163
We were discussing non-HDL-c, not what marker is the best… in exclusion of all others.
Here’s the study discussed by Sniderman.
I am not going to argue about what quote is representative of the article.
Ignore non-HDL-c if you wish. I am not.
2 Likes
ng0rge
#164
You better not! But all kidding aside, I just very carefully read the MR study that you (inevitably) posted, and yes it was very good and made a good argument. It does say-
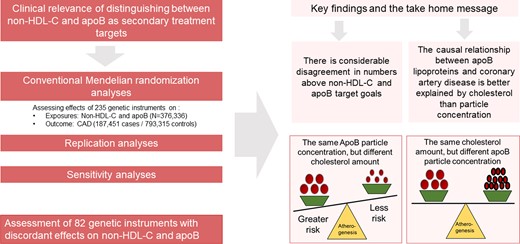
“Given the high correlation between non-HDL-C and apoB, it could be argued that distinguishing between the two biomarkers is not clinically relevant.” so the argument between them might be somewhat academic.
However you should read the opposing argument here (by Sniderman):
https://www.researchgate.net/publication/26726261_ApoB_versus_non-HDL-C_What_to_do_when_they_disagree
You need to download the PDF but it’s an easier read. It argues that in the majority of cases ApoB gives you a better measure and that it’s a more precise lab test. But, there is a rare case where non-HDL-C is better.
“However, in rare instances, non–HDL-C can be
positively discordant with regard to apoB if large numbers
of cholesterol-enriched chylomicron and VLDL remnant
particles are present. In this specific circumstance,
non–HDL-C or total cholesterol (TC), but not apoB, is the
valid index of atherogenic risk.”
So yes I agree that they are independent risk factors but generally correlated.
2 Likes
A_User
#165
No, not if your non-HDL-c is suboptimal.
That article is from 2009, I am not going to read it, the field has advanced a lot since then.
ng0rge
#166
You can find out all you need to know if you google “ApoB vs non-HDL-C”. And a good article to pick from that list is this 2021 article from Sniderman (the authority when ApoB and non-HDL-C are discordant):
https://academic.oup.com/clinchem/article/67/11/1440/6372218
His conclusion hasn’t changed since his 2009 article that I listed above. Non-HDL-C has been around a long time, it’s part of the standard lipid panel and it’s a much better measure of risk than LDL-C. The big push in lipidology is to get people to test for ApoB (and one time of Lp(a)) because in most cases (the exception I quoted above) ApoB is the best measure of risk and once you have that, you can forget about non-HDL-C. Despite what @A_User says, as Sniderman points out, in most cases it will be ApoB that will alert you to a problem that non-HDL-C didn’t show and not the other way around (rare).