Phosphoglycerate kinase 1 as a therapeutic target in neurological disease 2025
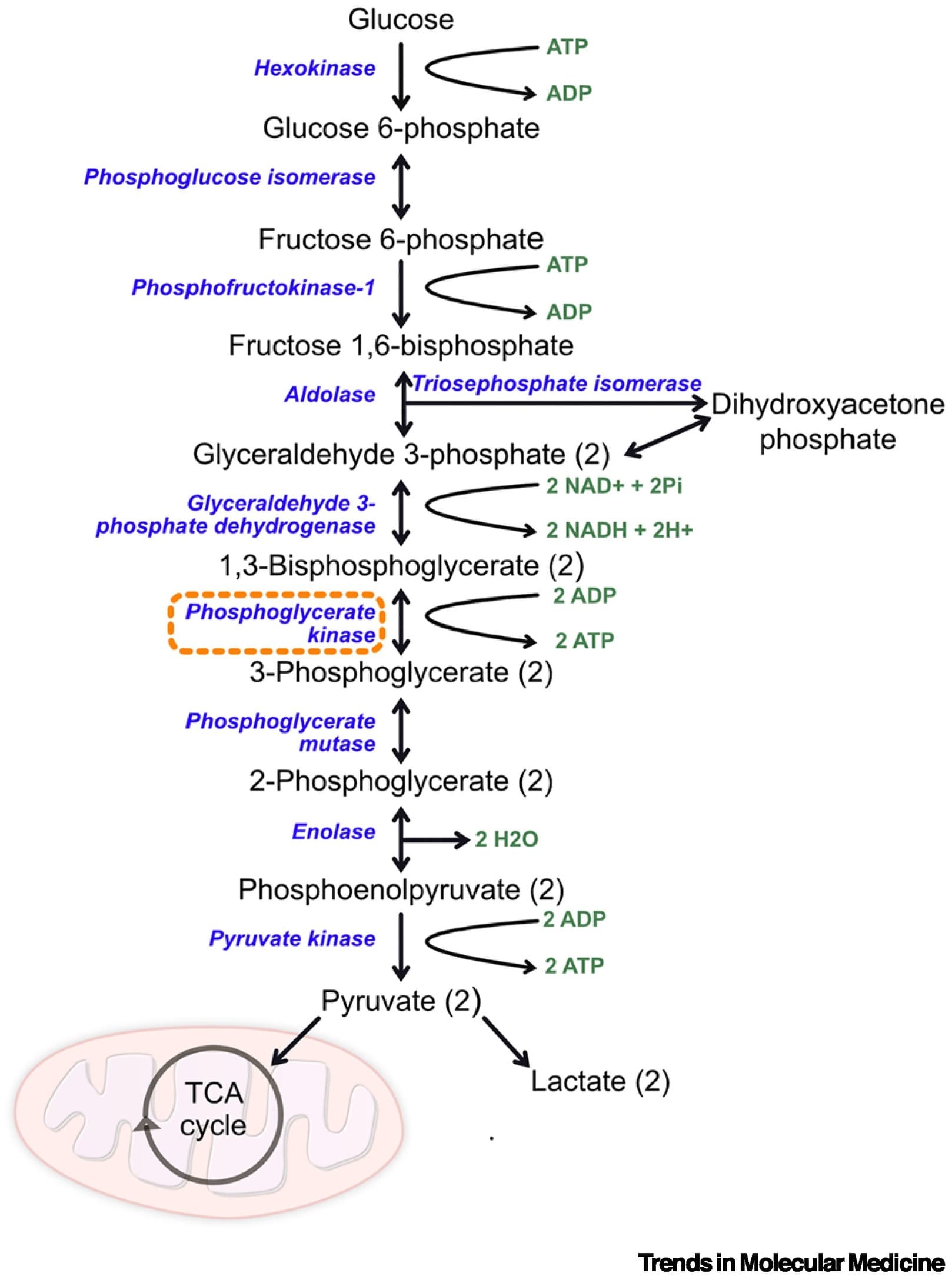
The glycolytic enzyme phosphoglycerate kinase 1 (PGK1) has emerged as a promising therapeutic target for both Parkinson’s disease (PD) and amyotrophic lateral sclerosis (ALS). Enhancing glycolysis represents an attractive approach because neurons are particularly vulnerable to dysregulated cell metabolism.
Although clinical trials of the PGK1 agonist terazosin are underway for PD and ALS, this compound can generate significant side effects, highlighting the need to identify alternative PGK1-activating strategies and compounds.
The potential benefits of increasing PGK1 activity in other neurological conditions are less clear. Further understanding of the noncanonical roles of PGK1 is needed to determine in which conditions increased activation may be beneficial.
Although it is unlikely to be a cure, upregulating glycolysis may be beneficial across multiple neurological diseases, and alternative approaches to activate this fundamental cellular pathway beyond PGK1 need to be explored. As always when targeting such core cellular pathways, there is a need for caution because the effect on normal cell function of increasing such fundamental cell processes is so far unclear. However, current data do suggest that targeting PGK1 and glycolysis has the potential to improve or delay the course of disease for many patients affected by neurodegenerative diseases, for which the therapeutic options are currently extremely limited (see Clinician’s corner). Considering this and the growing body of supporting evidence, the benefit of increased PGK1 activity in multiple neurological conditions is worthy of further preclinical and clinical investigation.
PGK1 activity is tightly regulated at the transcriptional, post-transcriptional, and post-translational levels [7]. HIF-1 is a strong regulator of PGK1 transcription, increasing its transcription in many hypoxic conditions [7,12,13]. PGK1 can also undergo a wide range of post-transcriptional modifications, such as phosphorylation, acetylation, succinylation, O-GlcNAcylation, crotonylation, or ubiquitination [7,14,15]. These could represent additional attractive therapeutic targets that have so far been studied mainly in the context of cancer [7].
The nervous system is particularly vulnerable to low oxygen levels, with hypoxia playing a key role in multiple neurological conditions. Under systemic hypoxic conditions, hypoxia-inducible factor (HIF)-1α is increased, which upregulates PGK1 as an adaptive response [59–62]. This increased expression of PGK1 along with other glycolytic proteins has been associated with better outcomes in hypoxic-ischemic encephalopathy in infants [63]. Increasing PGK1 activity with an agonist in mouse and cell models of acute hypobaric brain injury was neuroprotective and reduced the production of ROS. It was found that PGK1 that has translocated to the mitochondria could interact with tumor necrosis factor receptor-associated protein 1, which is a mitochondrial molecular chaperone that helps to regulate production of ROS [64]. PGK1 that has translocated to the mitochondria can also phosphorylate PDHK1, inhibiting mitochondrial pyruvate metabolism and ROS while also promoting cell proliferation [65]. PGK1 is also upregulated following TBI, with higher PGK1 levels being associated with improved prognosis in patients [66]. It has been suggested that PGK1 may help to regulate the process of ferroptosis after TBI, although its precise role in this is unclear.
It is worth noting, however, that increased PGK1 activity may not always be beneficial in this context. A mouse model of postoperative cognitive dysfunction induced with etomidate found that the increased expression of HIF-1α and associated increase in PGK1 resulted in increased levels of oxidative stress, with downregulation of HIF-1α being protective [67]. Moreover, an in vitro oxygen-glucose deprivation/reoxygenation model of ischemic neuronal injury revealed that the translocation of PGK1 to mitochondria occurring in hypoxic conditions was associated with a decrease in cytosolic PGK1, which was found to increase neuronal cell death [16].
The multiple roles of PGK1 outside of its primary role in glycolysis are still poorly understood and may explain some of the discrepancies observed. The degree to which PGK1 activity is increased also appears to be an important factor because intraperitoneal injection of low doses of PGK1 fused with PEP-1 to cross the blood–brain barrier reduced neuronal death in a gerbil hippocampal model of ischemia, whereas a higher dose was not found to be protective [68]. This supports previous work that showed a low dose of terazosin was protective and resulted in a lower infarct volume in a rat model of stroke, whereas a higher dose was not beneficial [69]. As discussed previously, the post-translational modifications of PGK1 may also play a significant role because hypoxia can result in a decrease in the lysine crotonylation of PGK1, and altered expression of succinylated PGK1 has been reported in a rat model of epilepsy even when total PGK1 levels were unchanged [14,15].
The evidence for targeting PGK1 activity in other neurological conditions, such as hypoxia and neuroinflammation, is mixed. Increased knowledge of the other roles of PGK1 apart from its canonical role in glycolysis will be key to understanding conditions where enhancing PGK1 activity would be appropriate.
@John_Hemming: bridging the gap between terazosin and hypoxia!