Well done John. Thanks.
The one study referenced looked to see if K2 improved mitochondrial function by increasing cardiac output. CO did, in fact, increase , but there was no change in stroke volume indicating that the increase was secondary to a heart rate increase.
It’s bizarre, that’s how I felt about it. We were even concerned that it might be excessive.
https://doi.org/10.1080/17512433.2019.1561102
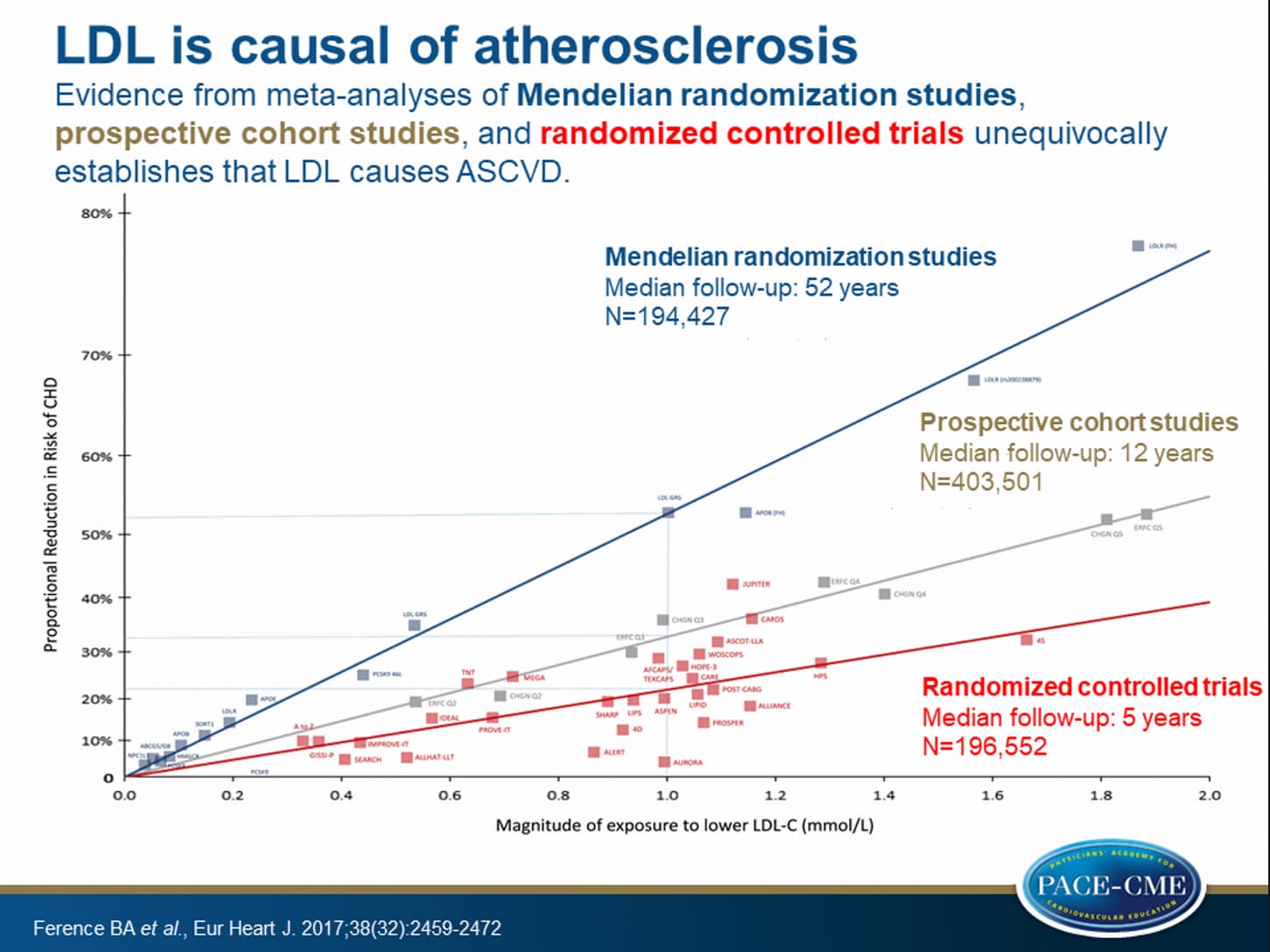
We propose, therefore, that clinicians would be better served to advise their patients to target lifestyle and dietary approaches which reduce their risk of developing CVD, rather than to prescribe treatments which lower LDL-C, such as statins, fibrates or PCSK9 inhibitors.
1 Like
I’ve done a lot of reading lately on ASCVD especially its causal relationship to dyslipidemia, but the more I read and understand the progression of ASCVD is fare more complex then just controlling dyslipidemia. ASCVD is primarily sterile inflammatory process where toll-like receptor (TLR) pathways is implicated. There were hypothesis that targeting TLRs to limit inflammatory disease might be a safe strategy, but TLR inhibitors increase the risk of non sterile infection too and this route was mostly abandoned and focus remained on lipid lowering strategies. There are some studies that some statins also affect and down-regulate TLRs and this might be one of benefits of (some) statins too, but statins primarily target LDL receptors. Since rapamycin showed good inhibition of TLRs (not in connection to ASCVD but in different other studies) it might prove to be an interesting prevention strategy after all. I also understand that lipid lowering strategy is useful in some degree as especially ox-LDL up-regulates inflammation and TLR pathways, so it is in a way causal. But since there will always be some atherogenic lipids present in blood serum the strategy to lower lipids with medicines is proving to be “quite unsuccessful” especially as primary prevention and there should be taken with a bit of doubt IMO. There are so many other factors that may cause sterile inflammation that focusing only on one end is really reductive and doesn’t stand chance to be successful. I do keep and open mind, but from what I know lipid lowering with medicines as primary prevention in healthy low risk individuals is ridiculous IMO. It has been propagated by Peter Attia, Tom Dayspring et al., but as much as I want to take it as a valuable and interesting point of view it is only one tile in the mosaic of the complex processes of ASCVD. I would like to believe that taking the “magic pill”, PCSK9i, statins or rapamycin will “magically” extend my life and fend off disease and aging. But it wont. It might not hurt, might help, but we do not know. And not knowing is what provokes the most existential fears in us. Maybe fearing less and living more is the way to do it.
2 Likes
A_User
#1732
The title of their paper is LDL doesn’t cause heart disease, and their argument is there isn’t an association. Spot the problem. They also just hand wave mendelian randomization away by saying it is an association.
2 Likes
I had Cleerly done on my recent CT…this was after a CAC of 154 and my doc wanting to get the imaging to know more…the doctor interpreting the scan said i had a blockage but he thought it was around 50% blocked…we got the Cleerly analyis back and it said 58% but it was clear that it could be higher…also it was in the LAD artery so i ended up having them go in through the vein in my arm and they did an actual measurement and it was actually 80% blocked…I ended up with a stent because of that…
The Cleerly did see some soft plaque and was able to do a better job than the doc of identifying soft vs. solidified.
2 Likes
LaraPo
#1734
What if lifestyle (diet, exercising, etc) is close to optimal, but lipids are still high? I’ve been a vegetarian for over 40 years with very active lifestyle and my cholesterol is still abnormal. What else should I improve in my “lifestyle” in your opinion that would void the need of taking statins? My doc doesn’t know the answer to this question, nor does my cardiologist, nor a few other specialists that I consulted.
2 Likes
RPS
#1735
You could try Berberine:-
- High levels of cholesterol or other fats (lipids) in the blood (hyperlipidemia). Taking berberine by mouth, alone or with other ingredients, might help lower total cholesterol, low-density lipoprotein (LDL or “bad”) cholesterol, and triglyceride levels in people with high cholesterol.
3 Likes
It all depends on risk assessment IMO. If my metabolic health would be in check (BP, BS, insulin, weight, triglycerides…), I would not be stressed, I would exercise, my diet would be reasonably healthy, my sterile inflammation (measured via hs-CRP) would be low, I wouldn’t smoke, drink or take drugs, my calcium score would be zero, I would not have family history of ASCVD… so my risk would be low or close to zero I would not take statins from what I know now and from what I heard from different doctors. But if my risk would be higher of course I would take statins or (depending on my age, form men the worst age is from 50-65, for women is lower if I remember it correctly) but would also keep above under control. Having the above under control is in what I know is fundamental since ASCVD is inflammatory disease having inflammation processes under control seems logical to me, but since lipids cause inflammation on it’s own there is just so much you can do on that end. ASCVD is a slow progressing disease. There might be more knowledge, prevention strategies and medicines down the road. The problem with statins are some open questions as they have effect on metabolic pathways and it is a group of drugs (not every statin is the same) so some might be more beneficial than others (e.g. with some there is increased risk of dementia). But since they do influence mitochondria function I would be very wary of taking statins perpetually for primary prevention. But don’t take this as advice what you should do, just another view.
2 Likes
A_User
#1737
“My risk isn’t high enough”
“My inflammation is low”
“No family history”
“I am not stressed”
“I exercise”
“My BP is good”
“My weight is good”
“Insulin is good”
“I don’t drink”
“I don’t smoke”
“I don’t take drugs”
“My calcium score is zero”
“My age matters, if I was older”
“My gender”
“There is going to be more knowledge, we don’t know enough”
“Down the road there is medicines”
“Problem with statins”
“Influence mitochondria function”
Nooo! It can’t be an indepentent risk factor! It can’t be!
8 Likes
A_User
#1738
Not stressed btw, that’s why I make sure to do everything perfectly because it’s very bad to lower ldl… Statins, those I am scared of, not my apoB… @scta123
Also have you had any side effects from statins @LaraPo ?
1 Like
LaraPo
#1739
According to my self assessment (using guidelines above) my risk for cvd is low. My cardiologist thinks the same. I have 3 negatives though: high lipids, 68 yo, transplanted kidney. Did not measure CAS but will soon. I’m trying to eliminate one out of 3 negatives (2 other are out of my control).
1 Like
A_User
#1740
Ignore the noise. Trust your doctors. Trust the science.™
(Not medical advice)
1 Like
You are once again presenting a strawman argument refuting an argument that is different from the one actually under discussion.
A comic diatribe by one man to A Ted audience doesn’t mean it’s true. Plenty of quacks and cuckoos have presented before Ted. That in itself lends no credence to his flawed argument.
That graph has been used by every uneducated idiot from here to Timbuktu to denigrate Ph.D.s.
Yes, I will trust the science until proven otherwise.
Thomas Dayspring
MD, FACP, FNLA - Clinical Lipidologist
@Drlipid
“A physiologic LDLc, meaning the level necessary for physiologic processes is 10-30 mg/dL. That does not mean everyone needs such a level, but rather there is zero danger from low LDLc”
6 Likes
A very interesting talk by a neuroscientist at Columbia University. Thanks Joseph.
I know many MD’s and PHD’s in various areas of science and we all agree that what we don’t know far exceeds what we know. The very best scientists are very humble and awed by the complexities of science and how little we truly understand.
3 Likes
It is difficult to discuss religion with deeply religious people.
I would never dispute smoking causes cancer as I would never dispute that LDL-C is one of the causal factors in ASCVD. Like with smoking also with high LDL-C not everyone develops the disease (for the matter of this argument I wont go into other diseases and problems smoking may cause). The main difference is, that smoking is directly causal and LDL-C is only one of the causal factors and lowering LDL-C does not correlate with lowering ASCVD risk while not smoking clearly does (I know someone could say, that even non smokers get cancer, but most of them are second hand smokers or live with other environmental causal factors). All I was saying is, that if my risk of developing ASCVD is less than 5% in next 10 years why would I take daily medicine that might lower my chance of ASCVD to less than 4%? There are so many unknown factors in ASCVD that for me personally and this is no advice to anyone is that it is not worth taking something that in best case would do very little to prevent ASCVD but in the long run might cause other metabolic problems?
I understand that there is some logic that there can be no ASCVD if there are no atherogenic particles present and we hope that physiological minimum levels are indeed low enough not to cause it. There are new medicines coming that might address LDL-C lowering strategy differently than statins and PCSK9i and might prove better at preventing ASCVD. But ATM I believe that lifestyle and taking care of metabolic health is more beneficial than taking statins (or even PCSK9i for that matter) for primary prevention in low risk individuals.
2 Likes
Very low LDL‐C levels <70 mg/dL was associated with increased risks of all‐cause, cardiovascular disease and stroke mortality .
https://www.ahajournals.org/doi/full/10.1161/JAHA.121.023690
Below probably is a good explanation for some aggressive behavior of Peter Attia et al. 

The association among dietary cholesterol, serotonergic activity, and social behavior was consistent with data from other species and experiments and suggested that dietary lipids can influence brain neurochemistry and behavior; this phenomenon could be relevant to our understanding of the increase in suicide and violence-related death observed in cholesterol-lowering trials.
1 Like
JDK
#1746
These correlation studies about statins are all nice and tidy, but i think it mostly comes down to glycation on LDL ans glycation caused inflamation of the arteries, we are flooded by sugary foods and drinks… and its well known how the sugar industri has stayed out of causation or correlation studies for decades $$ 
2 Likes
A_User
#1747
Because you’ve maybe not heard the argument. It is compounding. It’s decreasing lifetime risk. If you invest in index funds, most of the time you don’t make a lot of money in 10 years, but in 30 years or longer, there’s a difference. If you have 1000$ and it increases by 5% every year, you will have $1600 in 10 years. But you will have $18 600 in 60 years. It is not linear. The decrease in risk from year 0-10 means the next years will have even less risk, and so on, building on itself. It is like a “healing” process.
2 Likes