约瑟夫
#123
FWIW… Today 04/21/2022 I added/started taking French Maritime Pine Bark and Gotu Kola.
As in my opinion this is safer than taking statins.
1 Like
An interesting study talking about how mTOR activation increases cardio risk:
2 Likes
Good stuff RapAdmin
So where are we as of now?
- Rapamycin protects against age related diseases. The protection against CVD seems very related to mTOR inhibition leading to increased mitophagy and autophagy, both of which reduce atherosclerosis.
- The sweet spot dose for this effect may be 6 mg/ dose.
- Rapamycin May, under certain circumstances, increase serum lipid levels.
- The risk of LDL would appear to be U- shaped
https://www.nature.com/articles/s41598-021-01738-w
It is certainly not a case of “ the lower the better”.
- HDL also seems to be U shaped with a sweet spot of 40-60.
- Apo B seems to be relevant, though some studies show that it doesn’t add much, but other studies suggest that it may be the most important element. Ratio of ApoB/ ApoA-1 under 0.8 may be prognostic as well.
- Statins certainly are indicated in certain high risk circumstances, but come with a variety of side effects.
So trying to digest all of this, I personally believe that keeping my dose of rapamycin at about the 6-9 mg per week dose is about right for now.
I feel that rapamycin protects against atherosclerosis and CVD even in the face of some elevated lipids.
Since I don’t have other CV risk factors, I’ll check my lipids and will be content with an HDL in the 40’s, LDL up to 145 or so, and an ApoB under 100. I’ll use a variety of supplements along with diet and exercise to achieve those goals.
1 Like
- HDL also seems to be U shaped with a sweet spot of 40-60.
FWIW, Nir Barzilai in Age Later claims that HDL decreases with age & that the very old people he studied had HDL in the higher end of the range, whence he concludes they had much higher HDL at younger ages. The implication is that the U shape on HDL may not be as low as you are suggesting.
Without knowing the actual mechanisms, we are using a pretty blunt tool to guess at what the lipid levels actually mean. Maybe for some situations high HDL is a problem & for others it’s an advantage, depending on what else is going on.
That’s a good point Elizabeth, but the low point seems to be < 30. The sweet spot is 40-60. If someone has a high HDL at a young age, let’s say a level of90, then I’d be hard pressed to say that an HDL of say 25 could happen just based on aging.
MAC
#128
More “leucine” smoking gun.
Interestingly, they report on a minimum leucine concentration threshold re mTOR. They also speculate on fattier cuts of animal protein, as dual protein-fat/lipid atherosclerosis signalling.
“Our data support the notion that excessive ingestion of dietary protein raises circulating amino acids to levels that impact plaque macrophage mTORC1-autophagy signaling resulting in apoptosis. Using these concentrations as a guide, the lowest dose at which leucine can activate mTORC1, suppress autophagy, elevate mitochondrial dysfunction, and exacerbate macrophage apoptosis requires a concentration of at least 400 μM (Figure 8). This is indeed on par with circulating levels of leucine after ingestion of a high protein meal and supports the pathophysiologic link between dietary protein excess and hyperactivation of deleteriousmacrophage signaling. We found only certain amino acids (with leucine leading the list) to be potent activators of mTORC1 in macrophages. This raises the question of whether dietary proteins proportionally enriched in leucine could drive macrophage activation and atherogenesis. Interestingly, leucine content is highest in meats and lowest in vegetable and grain sources. Indeed, we observed leucine was not alone sufficient to induce macrophage apoptosis, but could synergistically enhance apoptosis with 7-ketocholesterol or cholesterol crystals. Since the presence of dietary lipids including cholesterol is essential for atherogenesis in both animal models and humans, it is intriguing to consider whether the high protein-induced atherosclerosis can be synergistically exacerbated in the setting of increased dietary cholesterol. This has relevance clinically since there is common consensus that “red meat” protein sources (which have high contents of both proteins and lipids) pose the most significant cardiovascular risk.”
Some other random interest papers on leucine:
Extrapolating to older folks at risk of sarcopenia who invariably are, on average, at the lowest level of muscular use. Pumping them with more protein above say a physiological minimum is likely doing nothing re muscle build/reserve. In the context of the dietary/longevity guidelines of higher protein for older folks. Resistance exercise?!
“High-dose leucine supplementation did not enhance gains in muscle strength and mass after a 12-wk RT program in young resistance-trained males consuming adequate amounts of dietary protein.”
“The capacity for critically ill patients to use ingested protein for muscle protein synthesis is markedly blunted despite relatively normal protein digestion and amino acid absorption.”
2 Likes
MAC
All very informative.
So increased protein = increased leucine = more mTOR activity = less autophagy/ mitophagy = atherosclerosis and CVD.
So would rapamycin be enough to inhibit all of that?
Maybe.
1 Like
MAC
#130
Yes I’d stack low protein and Rapamycin, and hit as many pathways as possible.
Of course, we’ve been mainly discussing cardiovascular diseases, but on the All Important parameter of total mortality risk it would seem that a total cholesterol of 210-240 may be ideal.
https://www.nature.com/articles/s41598-018-38461-y
2 Likes
MAC
#132
All cause mortality in 12 million + humans followed over 13 yrs that’s…that’s compelling.
220 is the absolute sweet spot. My 6 yr average TC is 217.
Many other similar all cause mortality studies across various other cohorts show a U curve in TC. And for the oldest cohorts, I’ve seen a tending to even slightly higher TC. There was large Japanese study that showed lower all cause mortality with higher LDL, I need to find it to share.
You wonder what’s happening on the low TC end, whether a side effect of illness not directly causative. Pharma?
1 Like
I posted the Japanese study earlier. The LDL sweet spot was about 144. Here’s a Denmark study where the sweet spot again is about 140 for LDL. Pretty clearly a U shaped
1 Like
Interesting since the Quest blood test results still recommend <100 ml/dL as does my current doctor. Am I missing something?
A meta-analysis of (130 070 patients)
Dec. 2021 is still using the low range as desirable.
Efficacy and safety for the achievement of guideline-recommended lower low-density lipoprotein cholesterol levels: a systematic review and meta-analysis
Quest
"LDL-CHOLESTEROL
mg/dL (calc)
Reference range: <100
Desirable range <100 mg/dL for primary prevention;
<70 mg/dL for patients with CHD or diabetic patients
with > or = 2 CHD risk factors.
LDL-C is now calculated using the Martin-Hopkins
calculation, which is a validated novel method providing
better accuracy than the Friedewald equation in the
estimation of LDL-C.
Martin SS et al. JAMA. 2013;310(19): 2061-2068
(LDL Cholesterol Calculations | Quest Diagnostics) "
1 Like
MAC
#136
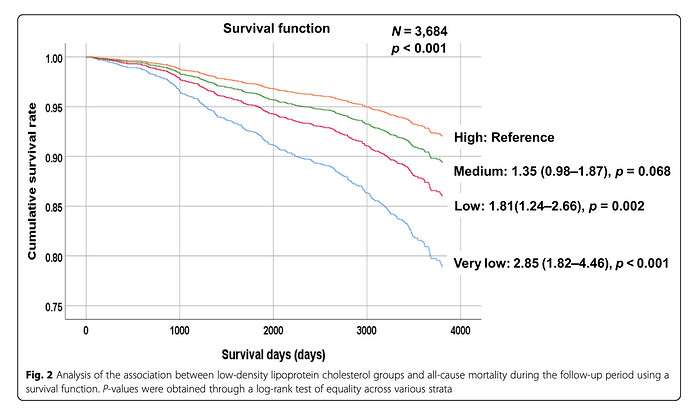
A Japanese study
Participants included 1610 men (63 ± 14 years old) and 2074 women (65 ± 12 years old) who participated in the Nomura cohort study conducted in 2002 (first cohort) and 2014 (second cohort) and who continued throughout the follow-up periods. Conclusions: There is an inverse relationship between LDL-C levels and the risk of all-cause mortality, and this association is statistically significant.
Very Low < 70
Low 70–92
Medium 93–143
High ≥ 144
Another. A large meta analysis. According to a recent systematic review of 19 cohort studies with more than 68,094 older adults, all-cause mortality was highest in the lowest LDL-C quartile group
Lack of an association or an inverse association between low-density-lipoprotein cholesterol and mortality in the elderly: a systematic review
“We sought PubMed for cohort studies, where LDL-C had been investigated as a risk factor for all-cause and/ or CV mortality in individuals ≥60 years from the general population. Results: We identified 19 cohort studies including 30 cohorts with a total of 68 094 elderly people, where
all-cause mortality was recorded in 28 cohorts and CV mortality in 9 cohorts. Inverse association between allcause mortality and LDL-C was seen in 16 cohorts (in 14 with statistical significance) representing 92% of the number of participants, where this association was recorded. In the rest, no association was found. In two cohorts, CV mortality was highest in the lowest LDL-C quartile and with statistical significance; in seven cohorts, no association was found. Conclusions: High LDL-C is inversely associated with mortality in most people over 60 years. This finding is inconsistent with the cholesterol hypothesis (ie, that cholesterol, particularly LDL-C, is inherently
atherogenic). Since elderly people with high LDL-C live as long or longer than those with low LDL-C, our analysis provides reason to question the validity of the cholesterol hypothesis. Moreover, our study provides the rationale for a re-evaluation of guidelines recommending pharmacological reduction of LDL-C in the elderly as a component of cardiovascular disease prevention strategies”
3 Likes
Informative video on this topic:
2 Likes
Seems pretty clear to me that there is a U- shaped curve for all cholesterol groups including TC, HDL, and LDL. Will ApoB also be U shaped?
Doubt that illnesses or malnutrition are driving the numbers down in all of these very large and well powered studies.
Also seems very possible that rapamycin, at least at some dosage, is atherosclerosis protective via multiple mechanisms independent of its lipid effects.
Is rapamycin driving lipids into higher cardiovascular risk territory, or actually lower all cause mortality territory?
1 Like
So far we’ve discussed the value of treating lipid levels as they relate to rapamycin therapy, the influence of various lipids on cardiovascular and all cause mortality rates, and the multiple studies demonstrating a U- shaped risk curve.
But what about rapamycin and associated hyperglycemia? Is that a risk worth an intervention?
If isolated hyperglycemia were a significant risk factor for either end organ damage, cardiovascular or all cause mortality, then surely strict glycemic control of the diabetic patient would be highly beneficial.
It’s not.
Multiple studies have shown no advantages to tight glycemic control
But what about controlling the more moderate glucose elevations that may accompany rapamycin usage? Let’s say an elevation that may place us in the pre diabetes territory . Is it worthwhile to attack those levels to prevent cardiovascular mortality with metformin, acarbose, etc.?
Again the answer seems to be No.
In fact, rapamycin has been shown to prevent retinopathy, nephropathy, and the neuropathy associated with diabetes. DM is a disease state in and of itself which leads to end organ damage and cardiovascular disease. It is not simply hyperglycemia.
1 Like
It’s interesting that the Levine biological age calculator does not use LDL-c or HDL in its calculation.
Here Michael Lustgarten makes the case the the Levine calculator is just as good as the Horvath calculator which uses a blood sample.
Quantifying Biological Age: Blood Test #3 in 2022
1 Like
The U shaped LDL cholesterol/mortality curve appears in observational studies, but importantly, does not seem to appear in interventional studies involving treatments to lower LDL; in fact, we see nothing but decreased cardiac events and either decreased or minimal effect on all-cause mortality when lowering LDL in such patients, certainly not increased mortality (even in statin users, despite elevated risk of diabetes, etc).
If such a U-shaped curve exists as a general rule and involved cause/effect rather than merely correlation, wouldn’t we expect to see significantly increased mortality whenever a drug is used to lower LDL, even to extremely low levels such as with statin + PCSK9 inhibitors? These folks aren’t dropping like flies; in fact, all evidence points to the fact that they’re thriving.
Implying a cause/effect relationship from observational data, when numerous experimental/interventional studies are already published, is a big mistake IMO.
At the very least, there may be two (or more) mortality curves – one for higher risk patients (the lower the LDL or apoB, the better, which appears to be true from mountains of evidence) vs low risk patients (maybe U-shaped or similar, but still no proven cause/effect relationship and why would someone with low risk be trying to lower his LDL down to insanely low levels anyway?)
4 Likes
This study raises some concerns:
Has anyone on long-term rapamycin been tracking their fasting insulin and HOMA-IR levels? Simply checking fasting glucose is not ideal when attempting to detect insulin resistance at its earlier stages.