At present, I believe there are still many questions to be answered.
- What is the target for lipid lowering? LDL, ApoB. Non- HDL, or oxLDL?
- Is it all just a numbers game, or does it mainly depend on other risk factors such as blood pressure, diabetes, etc?
3.Do we need to be careful of increasing all cause mortality with excessive LDL lowering?
- Are statins safe enough for primary prevention or are we better off considering berberine, Amla, and citrus bergamot which aren’t implicated in cognitive impairment?
- Is rapamycin protective enough to be a significant consideration in this decision?
2 Likes
Finally someone I totally agree with. Well said.
1 Like
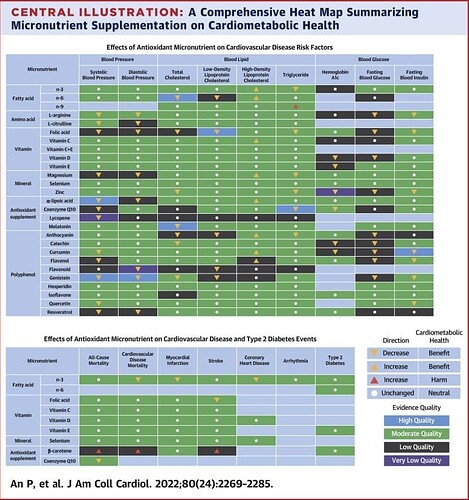
Other micronutrients that affect cardiometabolic health.
2 Likes
rivasp12
#1172
“The benefits of taking statins are inconsistent and often modest”
1 Like
rivasp12
#1173
Folate surprised me a little. Might be the homocysteine connection. The evidence for omega 3’s continues to build.
2 Likes
A_User
#1174
What conclusion can you draw from that study?
1 Like
Hard to believe that at one time people thought taking B carotene was a good idea. It really shortens your lifespan!
1 Like
rivasp12
#1176
The same conclusion that I draw from most of the studies. In the primary prevention the Absolute risk reduction of All cause mortality is very very low, if any. Not worth the side effects.
1 Like
A_User
#1177
Does it matter to you at all how long they were treated?
Because the MR studies show a larger, compounded benefit, over time.
1 Like
A_User
#1178
I don’t have access to the full paper, but I was going to ask how it was possible to find an ACM difference in a supplement trial, but then I realized it says the evidence is low quality. I don’t know what that means, so it hasn’t totally convinced me though.
2 Likes
rivasp12
#1179
Sure, it would be nice to have a multi decade study.
NHANES is an 18 year study , and again, the lowest LDL group had the highest all cause mortality rates, even after adjusting for Multiple variables. This isn’t an isolated study showing this disturbing trend.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8586008/
1 Like
A_User
#1180
So why aren’t people in statin or PCSK9 inhibitor trials dropping dead like flies? Or people with genetically low LDL levels? In fact, the opposite is happening.
Here’s a good article summarising the low ldl assosciation paradox, and it points to underlying metabolic disease. There’s even association studies showing the opposite effect, so what do you trust?
5 Likes
rivasp12
#1181
N HANES controlled for metabolic diseases and even cancer. The risk for low LDL continued.
1 Like
A_User
#1182
That is for diagnosed diseases, it probably is (based on the other evidence) an undiagnosed disease which is causing the low LDL which makes it associated with ACM. Undiagnosed cancer, for example. It is based on data from a survey. But the study did exlude a 3 year follow up which would reduce the reverse causation significantly.
rivasp12
#1183
The reverse causation explanation is just an unproven theory right now. In the meantime, there’s cause for concern about lowering lipids too much.
If you have risk factors for CAD, it’s very sensible to get your lipids down to a reasonable level, while being careful to not go too far until future data clears up some of this confusion.
You don’t want to risk all cause mortality while trying to prevent heart disease.
A_User
#1184
I just showed you possible explanations, I wasn’t trying to prove that it is. The mendelian randomization and randomized controlled trials prove that it is reverse causation. But you obviously don’t care about those, as that evidence has been posted many times in this thread.
2 Likes
rivasp12
#1185
I have no horse in this race. I understand that the studies are conflicting and the water is muddy.
Unlike you, I don’t yet have complete clarity on this issue, so I’ll continue to adhere to the very reasonable AHA guidelines on when to treat lipids for both myself and my patients.
I’ve posted Numerous studies on this thread . All cause mortality is all I care about in the final analysis. Absolute risk is far more important than relative risk.
2 Likes
“The overwhelming evidence demonstrates that deliberate pharmacological lowering of LDL-C does not increase cancer risk or all-cause mortality risk”
It is quite confusing, but the historic weight of evidence still indicates that for most people reduced LDL is better.
This video gives a good overview of a controversial subject.
3 Likes
rivasp12
#1187
The question is under what circumstances do we address LDL and how low May be too low for overall mortality risk. Far from clear.
1 Like