Keep thinking that.
Multiple studies are showing a U shaped curve.
It isn’t all just reverse causation.
Sensory impairment, infections, and even cancer are real risks with too low LDL.
All cause mortality is all that matters.
1 Like
Not at all. Side effects show up at any point, and sometimes decades after a drug is approved.
1 Like
Well, Lipitor has been in trials and use for three decades plus. Your argument is not compelling.
1 Like
CTStan
#1149
Given the U curve and mortality risk data, what would be a reasonable target for LDL. My target had been <70. Maybe below 90 but above 70? Best guess?
I saw a patient two weeks ago, 34 years old, who, after 1 year on a statin couldn’t remember what he had done just 30 minutes ago. No idea.
Completely resolved shortly after stopping it.
Tell him about the safety of decades of use. How many other cases are out there that just aren’t being reported by very busy doctors?
2 Likes
I’m not at all telling you to not take statins. I’m neutral about it. I’m presenting data that should make you consider how low you want your LDL to go. Is the present faddish notion of “ the lower the better”, justified? Or is it dangerous?
Off-topic. We were discussing the carcinogenic dangers of statins of which there is no compelling evidence. I don’t deny that statins have unpleasant side effects for many people, nor am I advocating very low LDL. The studies showing a U-shaped curve seem to indicate the best levels to aim for.
There’s evidence.
It’s totally subjective how compelling it is.
1 Like
A_User
#1155
You’re literally basing this on studies claiming an association, not causation. Correlation doesn’t mean causation. The causal evidence is pointing in the other direction, you have this backwards.
2 Likes
You’re right . The causal evidence for statins reducing the absolute risk of all cause mortality in primary prevention is close to zero.
3 Likes
A_User
#1157
Did they not show a reduction in ACM or was it just not statistically significant? If the latter it’s probably because of amount of participants/duration.
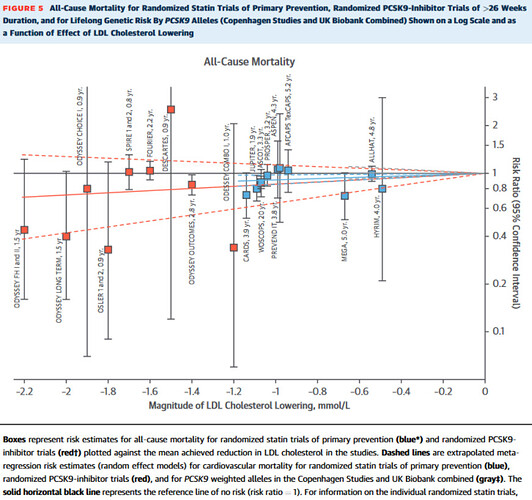
Genetic studies and PCSK9i didn’t reach statistical significance for ACM, but statin trials did show statistical significance for reduction in ACM.
When major studies are published in respected journals like JAMA and NATURE, and they keep showing the same trend of very low LDL associated with increasing mortality, these shouldn’t be just casually dismissed. This is particularly true if the same association keeps repeating itself after they control for multiple variables.
Association studies are inferior to RCT’s, but that doesn’t make them worthless.
zazim
#1159
There are numerous relational studies that indicate skipping breakfast increases mortality. Above a certain age, there is a strong correlation between a normal BMI and increased mortality. I don’t pay any of them any attention, however.
1 Like
I talked to him at a health show years ago in Las Vegas. He was on a mission to get the word out because his memory was affected until he got off statins.
1 Like
It is an interesting question as to whether statins affect memory.
1 Like
A_User
#1162
Even if we believe statins can affect cognition which there is no good evidence for IMO, (Peter Attia has three part series on this here)
You can take statins that are less likely to cross the blood-brain barrier, like hydrophilic statins rather than lipophilic. For example Crestor (rosuvastatin) and Pravachol (pravastatin). And you can measure desmosterol levels which might have a link to cognition / AD.
80% of Peter’s patients above 40 are on lipid lowering medications.
And there are other medications than statins that lower LDL-c like PCSK9 inhibitor or ezetimibe.
1 Like
rivasp12
#1163
Even apart from clinical case studies, there’s absolutely evidence for statins and impaired cognition.
1 Like
A_User
#1164
The effect in context:
In the general population (18-65) reaction time increases by 2.8 ms a year.
And the study found an increase of 0.067 milliseconds per 1 SD decrease (38.7 mg/dL) in LDL-C in total. So if you have 2 SD lower LDL-c you have 0.14 ms increase in reaction time. And HMCGR inhibition showed improved memory performance:
However, our finding of concurrent improved memory performance associated with the HMGCR instrument highlights the complexity of the HMGCR-cognition relationship.
Also I don’t know enough about the mechanism, but genetic HMGCR inhibition is in the brain as well? Statins need to cross the BBB otherwise it is in the periphery, and some statins are less likely to cross the BBB.
Also that the effect is so small is replicated with the polygenic nature of cognitive performance, 10 000 genes determine it in similar environments, all with very small effects in either direction.
This means that there must be at least thousands of IQ alleles to account for the actual variation seen in the general population. A more sophisticated analysis (with large error bars) yields an estimate of perhaps 10,000 in total.1
Each genetic variant slightly increases or decreases cognitive ability. Because it is determined by many small additive effects, cognitive ability is normally distributed, following the familiar bell-shaped curve, with more people in the middle than in the tails. A person with more than the average number of positive (IQ-increasing) variants will be above average in ability. The number of positive alleles above the population average required to raise the trait value by a standard deviation—that is, 15 points—is proportional to the square root of the number of variants, or about 100. In a nutshell, 100 or so additional positive variants could raise IQ by 15 points.
1 Like
It is quite a complex interrelationship and demonstrates really the intertwined nature of cellular metabolism.
Substantial reduction in expected atherosclerotic cardiovascular disease risk in the next 30 years is achievable by intensive lipid lowering in individuals in their 40s and 50s with non–HDL-C ≥160 mg/dL. For many, the question of when to start lipid lowering might be more relevant than whether to start lipid lowering.
4 Likes