I have recently been intermittently taking an Italian produced version of Red Yeast Rice which has Monacolin K in it which is lovastatin.
I am to be honest in a bit of a mood about my various lab results on LDL-C because they vary so much (including on the same sample of blood).
The last one (from a new lab) was 2.29 mmol/L and the previous one was 3.15 and then I had three on the same sample at 2.42, 2.2 and 3.01. I have a working hypothesis that the amount of LDL-C in a blood sample gradually reduces as time passes before the sample is tested. The threshold for concern in the UK is 3 mmol/L (116 mg/dL) which is why this is a bit more significant.
Hence I don’t know whether the RYR/Lovastatin is reducing LDL-C or C overall or it is simply a testing artifact.
Davin8r
#1104
Is that the argument? As we know, there are more tools than statins to lower/control LDL. Aside from keeping dietary saturated fat low, Attia is more of a proponent of PCSK9 inhibitors, as they have a cleaner mechanism of action and selectively lower ApoB in the circulation without affecting cholesterol synthesis. A cheap oral version could be a holy grail of sorts when it comes to CVD prevention, if/when started early enough.
2 Likes
rivasp12
#1105
It’s tricky. I thought that Peter was suggesting that if you reduce the ApoB to about 20 and maintain that level for life, then you’d essentially eliminate CAD as a cause of death, but maybe I’m mistaken.
Let’s say you have 100 twenty year olds and you give them PCSK- 9’s for basically forever. Half of them may be unnecessarily treated and subjected to side effects. But perhaps if you only treat the non zero CAC people? Or maybe also include 2 other risk factors?
2 Likes
Davin8r
#1106
He said if we gave PCSK9 inhibitors to everyone with elevated ApoB early in life, it would make CVD the number 10 killer in the world instead of #1. Of course it’s more of a thought experiment than anything, since that will never happen, but it would basically be replicating the Mendelian randomization LDL studies which show very low CVD incidence in those genetically blessed with low life-long LDL levels.
1 Like
rivasp12
#1107
Okay, I get it now.
Here’s an interesting hypothetical. Let’s say that you’re 55 with a family history of both parents having heart attacks or strokes in their mid eighties. Your CAC is zero. You take rapamycin.
Ordinarily, you’d be okay because the strong FH wouldn’t count as a risk. But you’re a rapamycin user and want to live to 120. So does that change the equation and suddenly the FH is very relevant?
1 Like
Davin8r
#1108
I’d say yes, unless ApoB (and Lp(a), for that matter) is already very low. Since CAC is 0, this person still luckily has an ideal window for prevention unless rapa is proven to be highly protective. In the current absence of data on protective effects of weekly or every-other-week rapamycin, I’d recommend that person keep ApoB as low as possible, BUT not necessarily with a statin. Would be great if potent PCSK9s were cheap and orally bioavailable.
Other factors I’d add – keep blood pressure below 120/80, keep visceral fat low, no smoking and regular Zone 2 and Zone 5 exercise training for maximal CVD prevention. Perhaps throw in regular mindfulness meditation practice as well. If all these other factors are on point but ApoB is still high, maybe the person could keep his risk low for another 60 years, but who knows?
3 Likes
A_User
#1109
I think Peter is pretty agnostic when it comes to ways of treating apoB. He uses a PCSK9 inhibitor and a statin. And I think he likes to start his patients on a statin.
- Because for some people to lower ApoB that much is trivial — Peter takes a PCSK9 inhibitor and a statin and he can basically eradicate it
Peter likes to start patients with rosuvastatin or pravastatin
A_User
#1110
It is an observational study and using LDL-c rather than apoB. If those 20 yr olds were treated, it seems very likely to me that all of them would have a negative CAC at 58. Since it is an observational study we don’t know why the low LDL-c group have a low LDL-c or how long they’ve had it too. The genetic or mendelian randomization studies exclude those confounding factors.
- From Allan’s interpretation of the literature, coronary calcification is associated with advanced disease
- If a patient has high apoB, the fact that their coronary calcium is negative doesn’t mean they don’t have a lot of disease and that the disease isn’t developing at a rapid rate; it could be there
There’s an argument saying, if the coronary calcium is negative, nothing’s going to happen to in the next five or 10 years
Maybe this is true; but the disease is developing and doctors can’t make the disease go away
Doctors can modify the effects of the disease, modify the consequences
1 Like
tongMD
#1111
What would be most interesting to me is future studies on gene-edited animals (with human liver) with all three ANGPTL3, PCSK9, and APOC3 - to see if there is an additive effect or not. It is likely the cost would be the same for knocking out all 3.
1 Like
rivasp12
#1112
The prognostic value of a CAC score of zero is well established for a period of at least 10 years, and one study suggested 22 years.
I have no idea that in this group that the disease is developing. I think that it’s more likely that the zero group has built in protective mechanisms .
1 Like
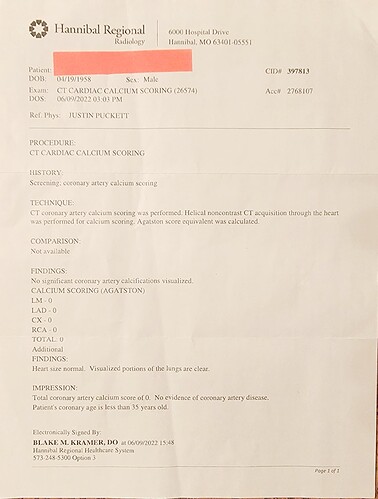
Agetron
#1113
As Peter Attia says - looks like the genetic lottery seems to have fallen in my favor at 64 years and 8 months. Zero score - I should get 10 to 22 years of no issues. Plus, on rapamycin for 2 years and 3 months what extra protection do I have? My veins have opened … varicose veins almost completely have vanished… something strong is happening within my arteries and blood vessels.
Also, one year ago on my CBC 10/29/2021 my LDL-C was 161; 6 months ago my LDL-C was 171; 4 months ago my LDL-C was 141; last week 11/10/22 making no dietary or supplement changes in the entire year my LDL-C is now 103. A 58-68 point drop and no medication or food changes. Just going to go with my Coronary Calcium Scan score of zero. Looks good and now my LDL-C 103 rating is good.
5 Likes
Nice result on the CAC, congratulation. Very good result indeed
On the LDL side, I would go with a direct method rather than a calculated one. And of course, ApoB should replace LDL-C, for a more realistic risk assessment.
2 Likes
A_User
#1115
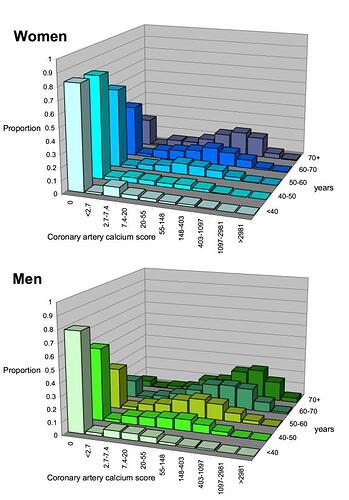
Disease has been delayed by some protective mechanism, might just be random luck too how the apoB particles have moved around. See the following two graphs, by age 70 most people have advanced atherosclerosis which is a positive CAC. Maybe that what Sniderman means the disease is present and developing. Unless you can keep apoB very low, it will for most of us. Of course with a positive CAC one can reduce events, stabilize plaques etc with statins that lower apoB a lot or LDL-c down to 20mg/dl like with a PCSK9i.
From Pletcher et al 2004. " What does my patient’s coronary artery calcium score mean? …"
EBT Coronary Calcium Scoring Guide, Alan Boyar 2013
4 Likes
rivasp12
#1116
Nice job Agetron. Probably a combination of great genes and behavior. I wouldn’t change a damn thing.
4 Likes
rivasp12
#1117
Large prospective study on CV risk factors according to age and relative risk factors.
Some notable takeaways:
- For the under 55 age, diabetes is the clinical disease most associated with risk.
- Hypertension is also associated with a 3.8 fold relative risk.
- The strongest risk biomarker is insulin resistance characterized by an elevated triglyceride/ Hdl ratio. Also a marker for inflammation. This was a greater risk than lipids or glucose.
- The risk factors attenuated with age.This doesn’t suggest that CV risk factors aren’t important in the elderly, but it emphasizes the importance of interventions in the younger age groups especially for insulin resistance and DM.
4 Likes
PDM
#1118
There have been cholesterol-lowering trials where the experimental (cholesterol-lowering) group had higher death rates. Minnesota Coronary Experiment and Sydney Diet Heart Study. Others as well.
1 Like
rivasp12
#1120
Always nice to hear from you Dennis and very happy for your much deserved success.
As to the topic, this is just one of several population studies showing similar trends. Even if we assume that the very low cholesterol group is reverse causation, wherein some form of underlying disease , like cancer, is driving the levels way down, it still doesn’t explain why the highest group has a lower mortality than the medium group.
3 Likes
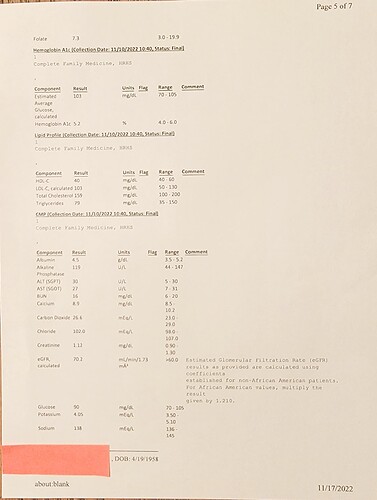
Agetron
#1121
Here is my ApoB from this week. Looks good too at 102.
2 Likes
CTStan
#1122
Even with your good health and low CVD risk, I would think below 90 would be a reasonable target for apoB.
In my own case, given my age and history of smoking, high CAC, and borderline glucose control, I have a more ambitious target of <60,
3 Likes