Davin8r
#1079
Truth is I still haven’t blocked anyone, but it’s good to know it can easily be done if/when desired. Anyway, done with sideshow, back to topic at hand…
1 Like
Thorin
#1080
“conclusively demonstrate causality” is too strong a statement.
We are not talking about gravity here; there remains significant uncertainty. Causality implies it always happens (A causes B; therefore, if A, we get B). Most likely, for heart disease, it is context dependent. Meaning, A doesn’t always cause B, but will cause it if conditions C, D, and E are present. But won’t if they are not.
1 Like
A_User
#1081
There isn’t uncertainty in the sense that A is necessary to be present for ASCVD.
C, D, E cannot cause ASCVD without A.
It is the necessary cause.
But, there is almost always statistical outliers for anything.
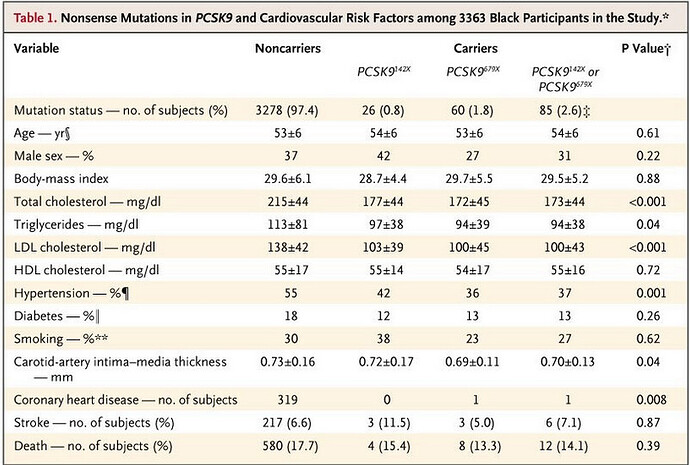
Here is an example genetic study with the LDL-c reduced, from Cohen 2006. As you can see there are still a significant proportion of people with normal LDL-c even with PCSK9 lowering.

There was a 88% of reduction in CHD. Rates of hypertension was almost comparable. The person who had CHD had an Lp(a) which is a form of apoB that is more atherogenic, at the 95th percentile, was obese, a smoker and had hypertension.
Lp(a) is another factor but it is genetically determined and is stable. There are some ways to lower it though via drugs and supplements.
3 Likes
Thorin
#1082
The comment I responded to was referring to LDL-c. FYI there are plenty of people in the hospital with heart attacks who have “normal” LDL-c. If your level were zero, yes, you would not have a heart attack, as you would be dead from something else already.
Given that we need a level above zero to survive at all, it is not clear what it means to say it is necessary to be present for ASCVD. You could say the same about Alzheimers, cancer, diabetes, etc.
Obviously I am NOT disputing that higher LDC-c is associated with more ASCVD. That is quite evident in the data we have. The quibble was limited to concluding that we’ve “conclusively demonstrate[d] causality” between LDC-c and ASCVD. That is too strong a statement in my opinion.
And, basically, you are agreeing when you say there are “almost always statistical outliers for anything.” Saying there are statistical outliers to LDC-C being causal to ASCVD is the same as saying it has not been conclusively demonstrated to be causal, in my view.
I know this blog is about Rapamycin so I will leave it there.
1 Like
A_User
#1083
Normal LDL-c around the 50th percentile is atherogenic, so that people who have heart attacks have a normal LDL-c is totally expected. What I mean necessary to be present is an apoB above 20 - 30 mg/dl, which is the levels we’re born with and isn’t atherogenic. Of course an LDL-c or apoB at the 5th percentile 60 mg/dl isn’t very atherogenic at all.
Higher LDL-c or apoB isn’t only associated with, it causes more ASCVD. That’s what the genetic studies are for, they exclude confounding factors like diet or lifestyle, or the lipid lowering medication studies.
I’m pretty sure you’re free to discuss LDL-c and ASCVD in this thread.
2 Likes
Thorin
#1084
The level of LDC-c neonates have is irrelevant here. The level of testosterone, growth hormone, or any number of other biomarkers found in infants is not necessarily relevant for determining appropriate levels for adults.
As far as I am aware, no human population studied has LDL-c levels in the vicinity of 20-30 mg/dL on average. I am not saying no humans have this level, but this is not a typical level found in any actual population to the best of my knowledge. So this is a red herring.
It is also quite evident that there are people with no heart disease who live a long time with high levels of LDC-c, and those with heart disease who had low levels (relative to other adult humans) their whole life. There is a lot of scatter in the data. As you said, there are “almost always statistical outliers.”
In any case, we may be arguing more about the meaning of words than biology here. If you think the data - which contains statistical outliers - has “conclusively demonstrated causality” you just think differently than I do.
I think it is highly suggestive of causality. LDC-c, as one of the causal factors that lead to disease, is the an excellent bet here. In my view it has not been “conclusively demonstrated” - i.e. - proven beyond any argument or discussion to the contrary.
2 Likes
A_User
#1085
I’m glad you’re questioning me on this topic. To be honest the apoB concentration of 20-30 mg/dl early is a thought experiment from Peter Attia where he thinks ASCVD will be a disease in the history books. Similar to how if everyone did a colonoscopy every day from the age of 30 there would be no colon cancer.
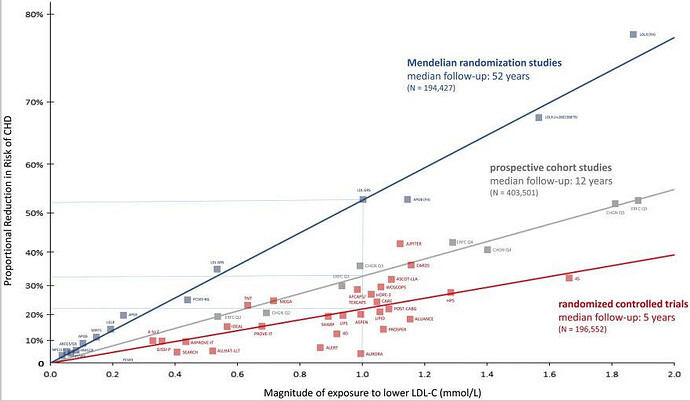
Here you can see the risk reduction between LDL-c and CHD. Since CHD is a very common disease, the abosolute risk reduction will be very large.
Lowering LDL-c even further in patient with low LDL-c leads to lower risk and no adverse events:
In summary, there is a consistent relative risk reduction in major vascular events per further reduction in LDL-C in patient populations starting as low as a median of 1.6 mmol/L (63 mg/dL) and achieving levels as low as a median of 0.5 mmol/L (21 mg/dL), with no offsetting adverse effects. These data suggest further lowering of LDL-C thresholds for initiating more intensive therapy, or simply targeting LDL-C at least as low as approximately 0.5 mmol/L or 20 mg/dL, would further reduce cardiovascular risk.
That’s basically the evidence I am basing this on.
(1) linear dose relationship between LDL-c and CHD from MR/RCT
(2) all the other evidence in the first paper I linked here, including mechanistic for those interested in that
(3) but also evidence lower LDL-c from already low LDL-c reduces risk.
You can see the studies and evidence for yourself and see if you want to care about apoB. I am very sold on it as you might imagine. You can find studies on why apoB is preferred over LDL-c if you are interested in that, Sniderman has a good review article about. But Peter Attia talks about it a lot.
2 Likes
rivasp12
#1086
Would this mean that a stressed out smoker with metabolic syndrome and a strong family history of heart disease would be out of the woods if he just corrects his APOb to the 30 level?
1 Like
A_User
#1087
David Sinclair started on a high dose statin when he was 29.
The thought experiment is based on a population starting in their 20’s, so unless they start treatment early, no not completely, but it will reduce their causal risk and possibly by a lot depending on where they started, and if they use statins it can stabilize plaques etc if they already exist. Their Lp(a) level matters too.
If they did start early, yes according to this thought experiment based on the evidence. However there are other factors to healthspan and longevity than just ASCVD.
I also think it’s a mistake thinking that ASCVD is an age-related disease when the evidence points to a time-based disease relating to apoB, so geroprotectors wouldn’t reduce ASCVD risk by the evidence presented, at least I wouldn’t bet on it. Signs of ASCVD is shown in young people too.
1 Like
rivasp12
#1088
Rapamycin could reduce inflammation, intimal thickening, foam cell formation, and reverse cholesterol transport to the point of very significantly lowering the risk of CAD .
In the primary prevention of the patient with very low CAD risk, lowering APOb has shown minimal absolute risk reduction of total mortality.
In the patients with multiple risk factors, lowering of atherogenic lipids certainly has a significant effect, but addressing the other risks, such as smoking,diabetes,obesity, would be necessary to greatly lower risk. Possibly reducing lipids to 0 would work, but that would require multiple medications and the role of lipid lowering, rather than say anti inflammation with statins, wouldn’t be totally clear.
1 Like
A_User
#1090
We don’t know.
What do you mean with low CAD risk, someone who is young? As age is the most significant risk factor for CAD, and I’ve said earlier why that is. I’d have to see the results of that study, most likely it’s because the study isn’t large enough or of a long enough duration to detect differences in total mortality.
More evidence that lowering LDL-c from already low LDL-c decreases events over 2.2 years, from Peter Attia discussion with Tom Dayspring, PCSK9 inhibitor study:
92 mg/dl to 30 mg/dl with hazard ratio 0.85 for primary endpoint, 0.80 for secondary endpoint.
1 Like
Arhu
#1091
He seems to be clueless about oral health judging from his tweets. I believe that any diet that’s bad for oral health is bad for the rest of our body too (and it is without doubt that these are just bad for our body period because our oral cavity is part of our body)
1 Like
Arhu
#1093
Just bullocks, we know not all root canals are successful, we know about the possibility of an apical delta but in reality more than 95% are successful and free from bacterial infection and we can tell especially after extraction (a small percentage just stinks but most don’t)
6 Likes
Davin8r
#1094
There are multiple CAD risk factors used when estimating 10 year risk, including coronary calcium score, lipids, blood pressure, smoking status, family history, etc.
IMO a very convincing argument put forth by Peter Attia in a recent podcast is that most physicians would say, in the face of a 40 year old with moderately high LDL or ApoB, if Ca score is low and other risk factors are low, that the patient’s cholesterol doesn’t need to be treated because calculated 10 year risk is very low.
Attia’s response to this is “Ok, your 10 year risk is low, but are you just trying to live to 50? Or do you want to live to 80 or 90 or 100? Because I’m more interested in your 30 year risk.”
We know that atherosclerosis has already started when a person is in his or her teens but doesn’t get bad enough to cause problems until literally decades later. Why would we expect, at the age of 50 or 60 or 70, that a statin drug given for 2 or 3 years that lowers lipids substantially, would reverse all that damage and eliminate risk? Or rather, why would we downplay the role of ApoB in CAD based on the relatively small absolute risk reduction seen in such short term studies? As Attia says, if a 25 year old shows up in the clinic with hypertension, it would be malpractice not to address it (not necessarily prescribe drugs), but all too often clinicians ignore high lipids at this early stage, when controlling lipids long term would actually have the biggest impact.
The take home message to me is that control of lipids likely has a huge impact BUT is slow and cumulative over years/decades, just as the buildup of arterial plaque is slow and cumulative over years/decades, and that it’s much harder to reverse than it is to prevent in the first place. Stabilization of existing soft arterial plaque to help prevent CVD events should be the immediate goal for patients with high plaque burden/high risk.
6 Likes
92 mg/dl to 30 mg/dl with hazard ratio 0.85 for primary endpoint, 0.80 for secondary endpoint.
Wow, that’s huge! (Sarcasm)
And, “The fight goes on”
1 Like
Bicep
#1096
I agree, and this does not include any other type of death like infection or pneumonia which would be protected by larger amounts of LDL.
2 Likes
Davin8r
#1098
Over a treatment period of 2 years. For a disease that took 40, 50, or 60 years to develop. If those lipids had been normalized decades ago instead of now, how much atherosclerosis and CVD events would these people be having?
4 Likes
I think you have just made an amazing case for preventative health. You need to start prevention early. Why would you think you can undo decades of damage over a few year time window after most of the damage has already been done?
Mother Nature has programmed us to live to about 80. We need to start interventions early (maybe some changes need to be done in our teens like eating healthy and exercising!) in order to go well beyond that. I wish I had thought about longevity earlier. I can only hope I am not too late. But, the progress so far has been encouraging!
8 Likes
rivasp12
#1101
Nearly half of patients with a very high LDL >190 had CAC’s of zero.
The argument is being made that if we treat all 20 year olds with statins for their elevated lipids, then we’ll be able to eliminate CAD. That one risk factor alone isn’t enough to justify such a draconian response.
5 Likes