Proof?
What we actually need is magic pixie dust. That’s what keeps our immune system working. There’s gotta be a Chinese in vitro study about this.
1 Like
Bicep
#2639
It says it reduced heart attack, stroke and fatal heart disease by one third. I didn’t read the actual study. The article doesn’t mention ACM or any other cause of mortality. They said it was about making sure it was safe to lower LDL, did they check ACM?
A_User
#2640
And as shown in the study I posted earlier, it is braindead to have ACM as the goal post as it requires a 25 x larger study than necessary.
Having low LDL-C levels with the accepted norms is good
The is no proof that having lower than this provides any additional benefits.
You should have pointed to the paper itself, not some communications major’s interpretation of the paper.
The study itself shows diminishing returns as LDL levels get lower. The is nothing in the paper that shows any benefits for LDL levels outside of the lower norm as measured by labs.
“LDL-C of ≈70 mg/dL, a further 20% reduction in LDL-C translates into a 6% to 7% lower risk of MACE. However, the question remains as to whether the additional percentage reduction in LDL-C (of 50% to 60%) and even lower on-treatment LDL-C level (<50 mg/dL) that can be achieved by adding a PCSK9 inhibitor to a statin will be associated with a lower risk of MACE.”
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.116.024604
1 Like
A_User
#2642
That is from previous results, if you keep reading it shows the benefits, in graphs as well.
L_H
#2643
It was blinded.
The fda audit of the Fourier study was unblinded, it’s still a blinded trial. Unblinded validation checks don’t render a study unblinded.
I think it’s clear that you hadn’t read the research properly, and are clinging to an argument for the sake of it. Its ok to change your mind now you’ve read it properly.Or do you still think the doctors were “Rogue”? 
A_User
#2644
We will have to agree to disagree then, and that is fine. 
L_H
#2645
That study is more convincing. And if I had cardiovascular disease i might be tempted to use a PCSK9i to get super low.
But I agree that “It is important to note that, although adverse consequences of very low LDL-C were not identified in these trials, the long-term effects of very low levels of LDL-C induced by PCSK9 inhibitors are unknown.”
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.116.024604
Neo
#2646
Thanks L Hayes
This is an area where I feel Peter Attia has both the right synthesis/read and where his resources have been very valuable
He had a good chapter in his book (and you may want to read the chapter Medicine 3.0 first)
Here is one place to start: On how early and aggressive lowering of apoB could change the course of ASCVD
He also has a great set of episodes on the drive about this with Tom Dayspring and others - and the shownotes have many of the key papers. You may have to me a member to access some of the shownotes (it’s not that much and may be worth it for a few months or a year).
Two other sources are
3 Likes
L_H
#2647
That’s great, thank you, very helpful. his target for apoB of <60 mg/dl exactly corresponds with my own target. Always comforting!
I’ll be very interested to hear if he and dayspring start aiming lower.
2 Likes
A_User
#2649
Cardiovascular disease is pretty much solved, so I don’t think there is much more to discuss in this thread!
Onto greater things!
Davin8r
#2650
Didn’t you say your calcium score is concerning? If it’s above 0, then you do have cardiovascular disease to one extent or another.
2 Likes
BTW, if anyone is interested in Bempedoic Acid, Jagdish and other Indian vendors sell it incredibly cheap! I just bought a batch of 200 tabs and will try it out when I get the meds at the new year.
Here’s his pricing:
1- Glycomet Tablet SR , Metformin 500mg = 0.6 USD for 10 tablet.
2- Ezedoc 10 Tablet Ezetimibe (10mg) = 2.4 USD for 10 tablets.
3- Brillo 180mg Tablet , Bempedoic acid (180mg) = 3 USD For 10 Tablets.
5 Likes
L_H
#2652
No, not me. (Extra characters)
scta123
#2653
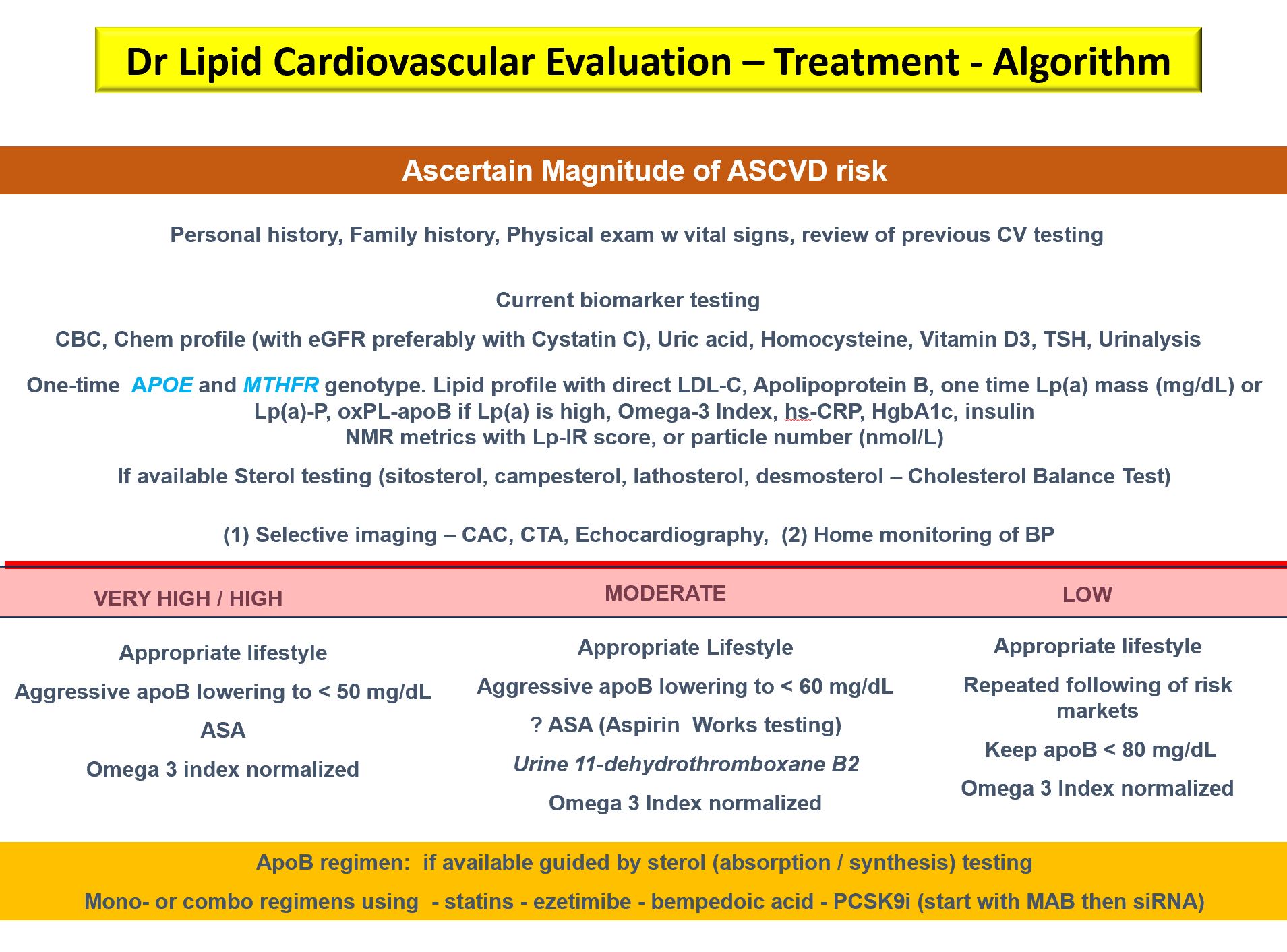
I think the aggressive lowering of apoB is over generalized. This is dependent on you ASCVD risk. LDL-C and by extension apoB are poorly associated with ASCVD on its own and they matter most in your younger years not when you are older. I am attaching again Tomas Dayspring’s treatment algorithm where is clearly seen that low risk individuals should aim for apoB below 80, but high risk individuals should aim for drastically lower apoB below 50. The absolute numbers in risk reduction for low risk individuals does not warrant the possible side effects of aggressive lipid lowering in low risk individuals.
3 Likes
A_User
#2654
There isn’t any side effects for most people.
That’s why they are longevity drugs.
I am quite certain that if you start taking a statin, you will be healthier, not unhealthier, overall and have a net benefit. And that is what matters.
I will soon go back on statins but I will measure my apoB before and liver markers, I will also try to eat more of a Med diet, then see what rosuvastatin does. I also have atorvastatin which I could try. Later on I can add ezetimibe.
scta123
#2655
Some people can’t tolerate statins (10-20%, some studies show even greater numbers up to 40%), for some they may pose increased risk of dementia, they also increase the oxPL-apoB, a more atherogenic form of of apoB, they can aggravate blood sugar control (another risk factor in ASCVD) etc. Ezetimibe works best in over absorbers not over producers (and you get similar benefit from soluble fiber which do give other benefits as well). PCSK9i are lacking clear safety information, Bempedoic Acid I haven’t really looked in depth. Fibrates seem interesting, especially Bezafibrate, that might reduce atherogenic particles count but not LDL-C in great amount but again there is no clear safety information.
IMO all depends on your risk assessment. If you are medium or high risk you should probably do something besides lifestyle, but low risk and keeping apoB below 80 is the most rational thing to do. You need to understand that Peter Attia is a medium/high risk from what he shared about himself and his personal actions should not be generalized to everyone. But saying that probably being low risk is an exception rather than rule in the real world. And even keeping apoB below 80 takes some effort.
4 Likes
A_User
#2656
I don’t believe in anything of that except that some can’t take them because of muscle side effects, increase in blood glucose, and liver enzymes. Two of which are objectively measurable, all of which are reversible, and rare.
They are longevity drugs and you will probably have a net benefit from taking them. It will probably increase both your health- and lifespan.
1 Like
It’s a sensible way of thinking. As a thought experiment, if I happened to find my apoB was very low (not due to intervention) I wouldn’t look for a way to increase it. I’m not worried about low apoB unless something shows up in my heath that is caused by low apoB. However if I am taking medications to lower apoB to very low levels, then I’d have to weigh the side effects of the medications against the incremental benefit of VERY low vs merely low apoB. If I had no side effects, then I wouldn’t be worried. At this time I am not worrying about any unknown, unseen, unfelt theoretical side effects other than the worry of too many simultaneous chemicals.
5 Likes
A_User
#2658
Exactly, and for most people, this will be the case.
Statins also decrease inflammation (CRP), and is associated with reduced rates of depression, meaning they can improve mood.