Waiting for Monday:
推特
See new Tweets
Conversation
Gil Carvalho MD PhD
@NutritionMadeS3
Coming this Monday on Nutrition Made Simple: Red Yeast Rice, phytosterols and other cholesterol-lowering supplements.
Do they work? Are they worth it? Are they safe?
A new trial suggests no supplements are effective over a placebo
A look at the research and the implications
1:40 PM · Nov 12, 2022
·Twitter Web App
2 Likes
Yes, the res yeast rice supplements made in the USA would have no effect as the FDA makes them remove the effective ingredient! 
I think Gil Carvalho MD Ph.D. is smart enough to take that into account.
We will just have to wait to see what he says. In any case, if U.S. red yeast rice has the effective ingredient removed there is no good reason to buy it or take it.
Of course, we could take almost any natural compound, however ineffective, and promote it as an elixir of health, and up to 40% of people taking it would swear by it due to the placebo expectation effect.
3 Likes
Davin8r
#1067
Consumerlab just did an analysis, and while some brands don’t have any lovastatin, some do. Cholestene has 7.5mg lovastatin per capsule, for instance. I do wonder, however, if the researchers chose one to test that was knowingly or unknowingly low or absent of lovastatin.
2 Likes
The FDA has issued an edict that lovastatin Monocolin K MUST be removed from red yeast rice supplements due to the fact is is a prescription drug. So any supplement that has lovastatin in the USA is technically illegal. Therefore red yeast rice supplements are useless (or illegal) if they were produced in the USA.
1 Like
A_User
#1070
Around 500 mg berberine a day and using more canola oil instead of olive oil reduced my apoB by 24% to 55 mg/dl. I’ve added around 0.8 mg of rosuvastatin three times a week now. There are studies only 1 mg a day reduced LDL-c by around 30%: Effect of rosuvastatin on low-density lipoprotein cholesterol in patients with hypercholesterolemia - PubMed. Ezetimibe also works in lower dosages:

“Statins are the most powerful longevity drugs available”:
2 Likes
Davin8r
#1071
Yes, the FDA has been complaining about RYR for decades but hasn’t ordered a RYR product off the market since 1998. It seems RYR manufacturers have been skirting the law by not listing monacolin levels on the label and not making claims about heart disease or cholesterol. So far, it’s worked but of course that could change.
1 Like
Davin8r
#1072
Thanks! Learning that I can block obnoxious users is the first, only, and last useful info I’ve learned from you on this site.
4 Likes
约瑟夫
#1073
FWIW
Make your own red yeast rice.
2 Likes
You may be right. But then how do you know which RYR supplement is useful or useless?
I have this image of each of you blocking the other. 
4 Likes
Davin8r
#1076
A membership has been worth every penny of my hard-earned money.
3 Likes
Davin8r
#1077
All I did was politely ask (on another thread) where he’s getting his info. Apparently, this blew a brain circuit.
3 Likes
I wasn’t trying to throw shade on anyone. I thought the symmetry amusing. 
2 Likes
Davin8r
#1079
Truth is I still haven’t blocked anyone, but it’s good to know it can easily be done if/when desired. Anyway, done with sideshow, back to topic at hand…
1 Like
Thorin
#1080
“conclusively demonstrate causality” is too strong a statement.
We are not talking about gravity here; there remains significant uncertainty. Causality implies it always happens (A causes B; therefore, if A, we get B). Most likely, for heart disease, it is context dependent. Meaning, A doesn’t always cause B, but will cause it if conditions C, D, and E are present. But won’t if they are not.
1 Like
A_User
#1081
There isn’t uncertainty in the sense that A is necessary to be present for ASCVD.
C, D, E cannot cause ASCVD without A.
It is the necessary cause.
But, there is almost always statistical outliers for anything.
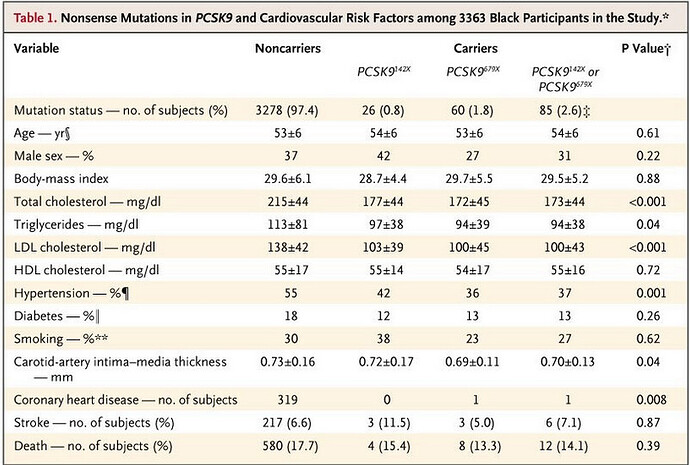
Here is an example genetic study with the LDL-c reduced, from Cohen 2006. As you can see there are still a significant proportion of people with normal LDL-c even with PCSK9 lowering.

There was a 88% of reduction in CHD. Rates of hypertension was almost comparable. The person who had CHD had an Lp(a) which is a form of apoB that is more atherogenic, at the 95th percentile, was obese, a smoker and had hypertension.
Lp(a) is another factor but it is genetically determined and is stable. There are some ways to lower it though via drugs and supplements.
3 Likes
Thorin
#1082
The comment I responded to was referring to LDL-c. FYI there are plenty of people in the hospital with heart attacks who have “normal” LDL-c. If your level were zero, yes, you would not have a heart attack, as you would be dead from something else already.
Given that we need a level above zero to survive at all, it is not clear what it means to say it is necessary to be present for ASCVD. You could say the same about Alzheimers, cancer, diabetes, etc.
Obviously I am NOT disputing that higher LDC-c is associated with more ASCVD. That is quite evident in the data we have. The quibble was limited to concluding that we’ve “conclusively demonstrate[d] causality” between LDC-c and ASCVD. That is too strong a statement in my opinion.
And, basically, you are agreeing when you say there are “almost always statistical outliers for anything.” Saying there are statistical outliers to LDC-C being causal to ASCVD is the same as saying it has not been conclusively demonstrated to be causal, in my view.
I know this blog is about Rapamycin so I will leave it there.
1 Like
A_User
#1083
Normal LDL-c around the 50th percentile is atherogenic, so that people who have heart attacks have a normal LDL-c is totally expected. What I mean necessary to be present is an apoB above 20 - 30 mg/dl, which is the levels we’re born with and isn’t atherogenic. Of course an LDL-c or apoB at the 5th percentile 60 mg/dl isn’t very atherogenic at all.
Higher LDL-c or apoB isn’t only associated with, it causes more ASCVD. That’s what the genetic studies are for, they exclude confounding factors like diet or lifestyle, or the lipid lowering medication studies.
I’m pretty sure you’re free to discuss LDL-c and ASCVD in this thread.
2 Likes
Thorin
#1084
The level of LDC-c neonates have is irrelevant here. The level of testosterone, growth hormone, or any number of other biomarkers found in infants is not necessarily relevant for determining appropriate levels for adults.
As far as I am aware, no human population studied has LDL-c levels in the vicinity of 20-30 mg/dL on average. I am not saying no humans have this level, but this is not a typical level found in any actual population to the best of my knowledge. So this is a red herring.
It is also quite evident that there are people with no heart disease who live a long time with high levels of LDC-c, and those with heart disease who had low levels (relative to other adult humans) their whole life. There is a lot of scatter in the data. As you said, there are “almost always statistical outliers.”
In any case, we may be arguing more about the meaning of words than biology here. If you think the data - which contains statistical outliers - has “conclusively demonstrated causality” you just think differently than I do.
I think it is highly suggestive of causality. LDC-c, as one of the causal factors that lead to disease, is the an excellent bet here. In my view it has not been “conclusively demonstrated” - i.e. - proven beyond any argument or discussion to the contrary.
2 Likes