What’s slightly odd about the movements when rapa was high in serum is that when you look at LDL-C the ratio between LDL-C and Lp(a) seems to vary
1 Like
nikney
#173
It is probably an RNA-based drug. It is a revolutionary drug that reduces lipoproteina levels by an incredible 90 percent by suppressing the gene region that synthesizes lipoproeina. Eli Lilly may have developed this drug by using artificial intelligence. If we consider that the biggest cause of death in the world is vascular diseases due to atherosclerosis, it will create an incredible increase in the average human life span.
Neo
#174
Probably largely genetic I’d assume as this is very genetically driven
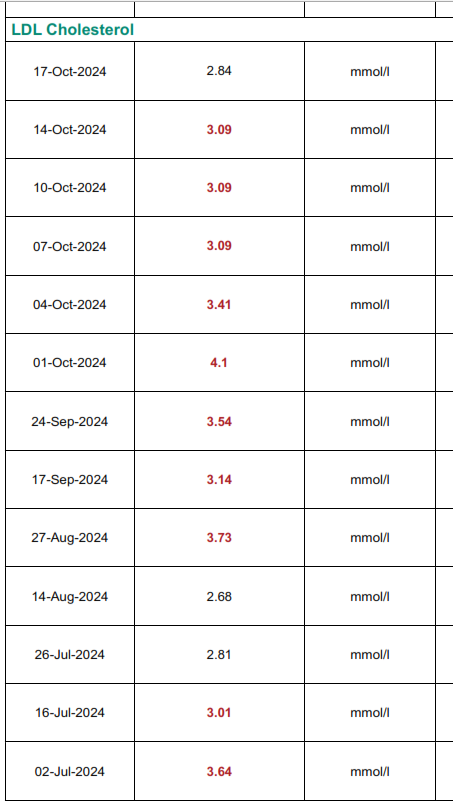
This is where I suffer from not having a baseline for this biomarker. I have been doing various biohackingy sort of things since about 2019 although initially it was a scattergun approach and only started doing blood tests in 2021. (and only 1 in 2021 and it was not broad enough).
Neo
#176
Have you done holistic DNA testing - you could see if you have the “right” version of LPA, etc
adssx
#177
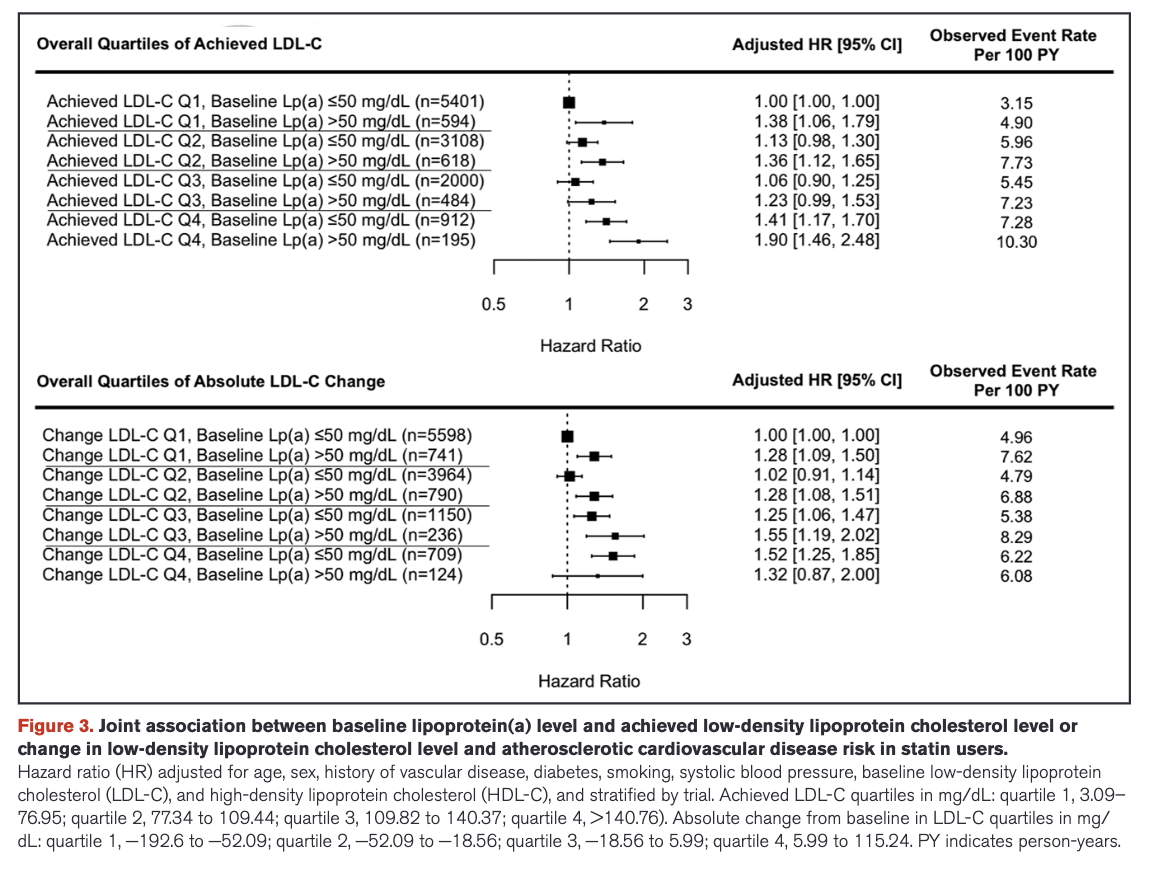
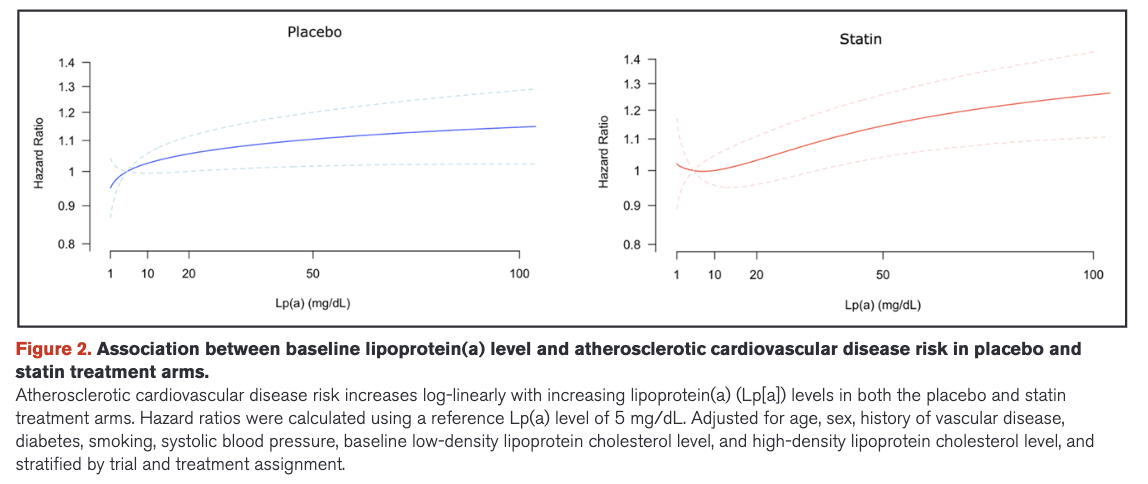
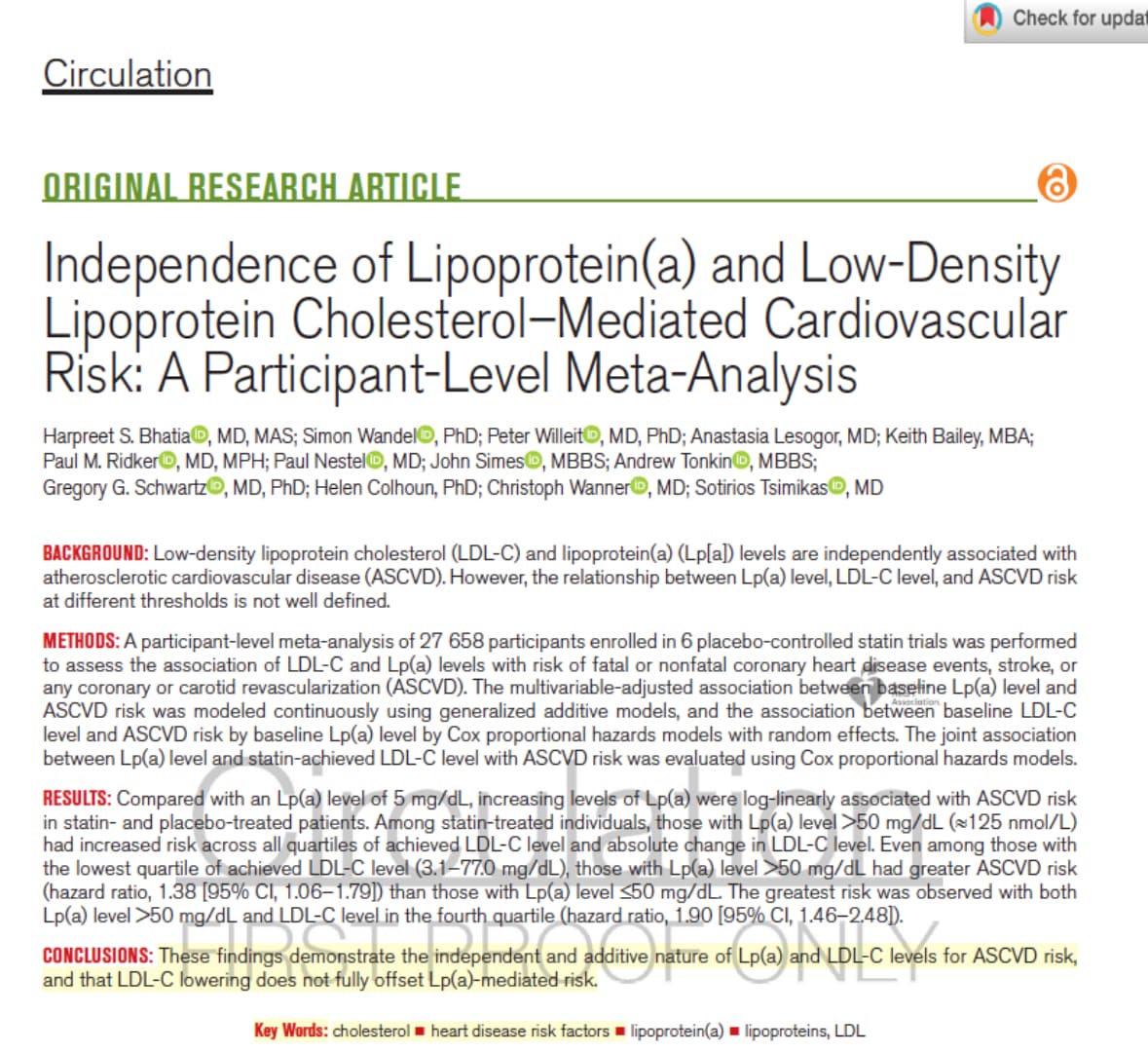
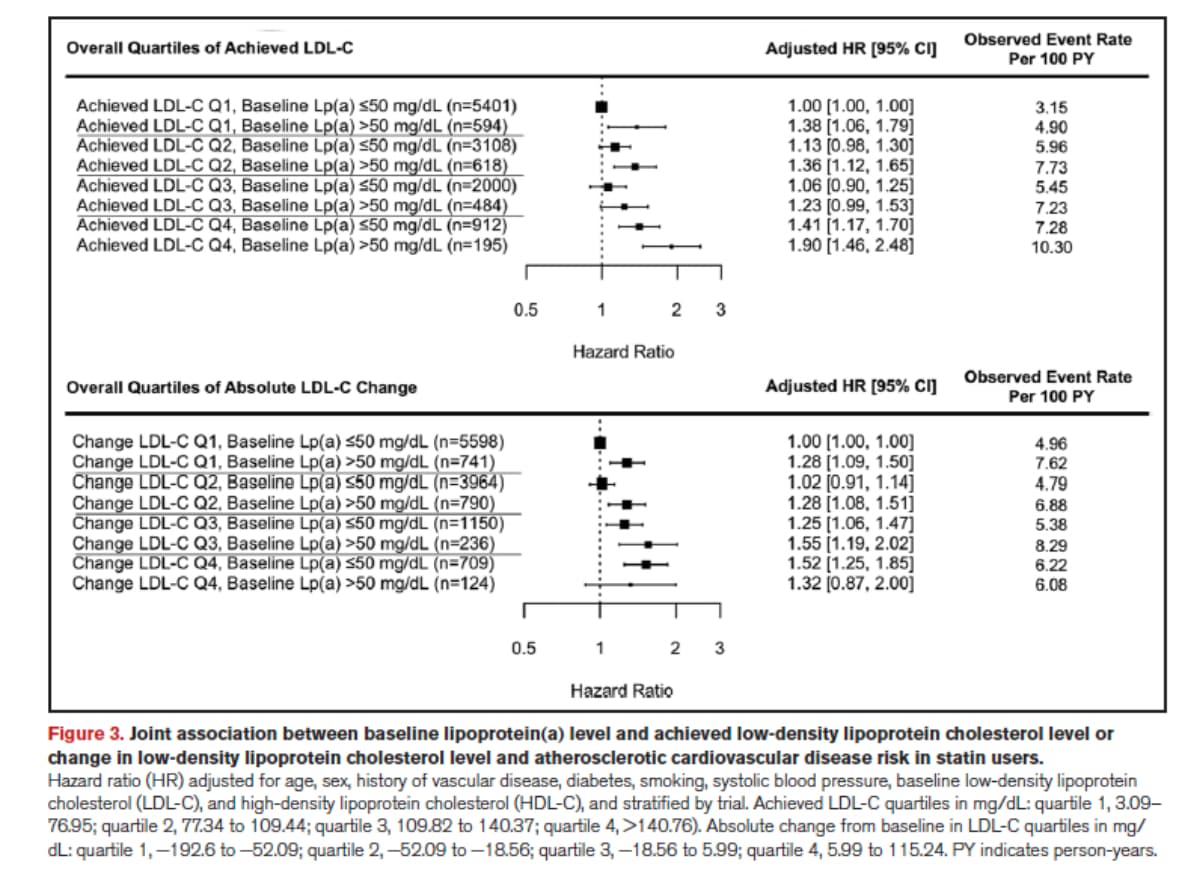
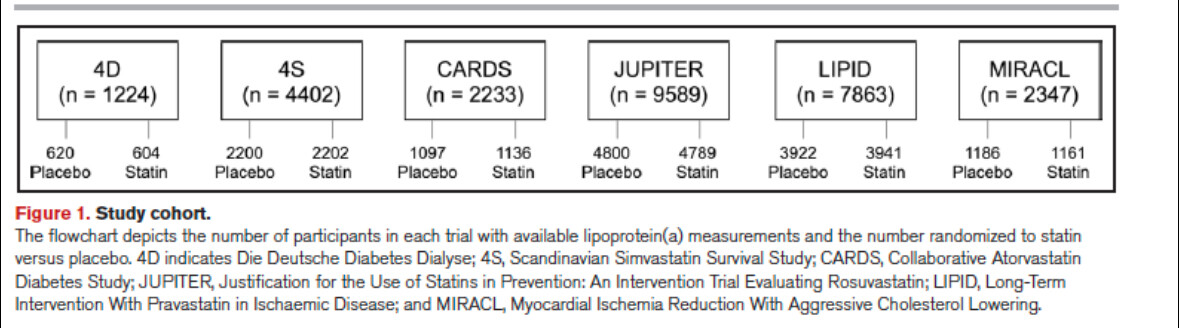
Independence of Lipoprotein(a) and Low-DensityLipoprotein Cholesterol–Mediated CardiovascularRisk: A Participant-Level Meta-Analysis 2024
These findings demonstrate the independent and additive nature of Lp(a) and LDL-C levels for ASCVD risk, and that LDL-C lowering does not fully offset Lp(a)-mediated risk.
3 Likes
Davin8r
#178
Which makes sense if a major mechanism of Lp(a)'s increased risk is mediated by excess platelet adhesion/thrombosis. Hoping my plavix continues to do its job!
1 Like
I find I have LPA data, but cannot tell what that means in terms of whether or not it is the right version. Is there a good online way of getting this from the raw data?
Neo
#180
Some of those platform are discussed here I think, and if not you can ask the people who know about it on that thread:
drfawn
#181
Are they still accepting people with high LP(a) into their trials? If so, how do I sign up?
Neo
#183
2 Likes
This tells me that you need to lower Lp(a) in addition to LDL. Low LDL doesn’t reduce risk to 0 by itself, but it still helps. I guess I need an Lp(a) test too to really find out where I stand.
An Lp(a) greater than 50 is considered the highest risk though.
1 Like
adssx
#185
Posted just above  New Lp(a) lowering drug - #177 by adssx
New Lp(a) lowering drug - #177 by adssx
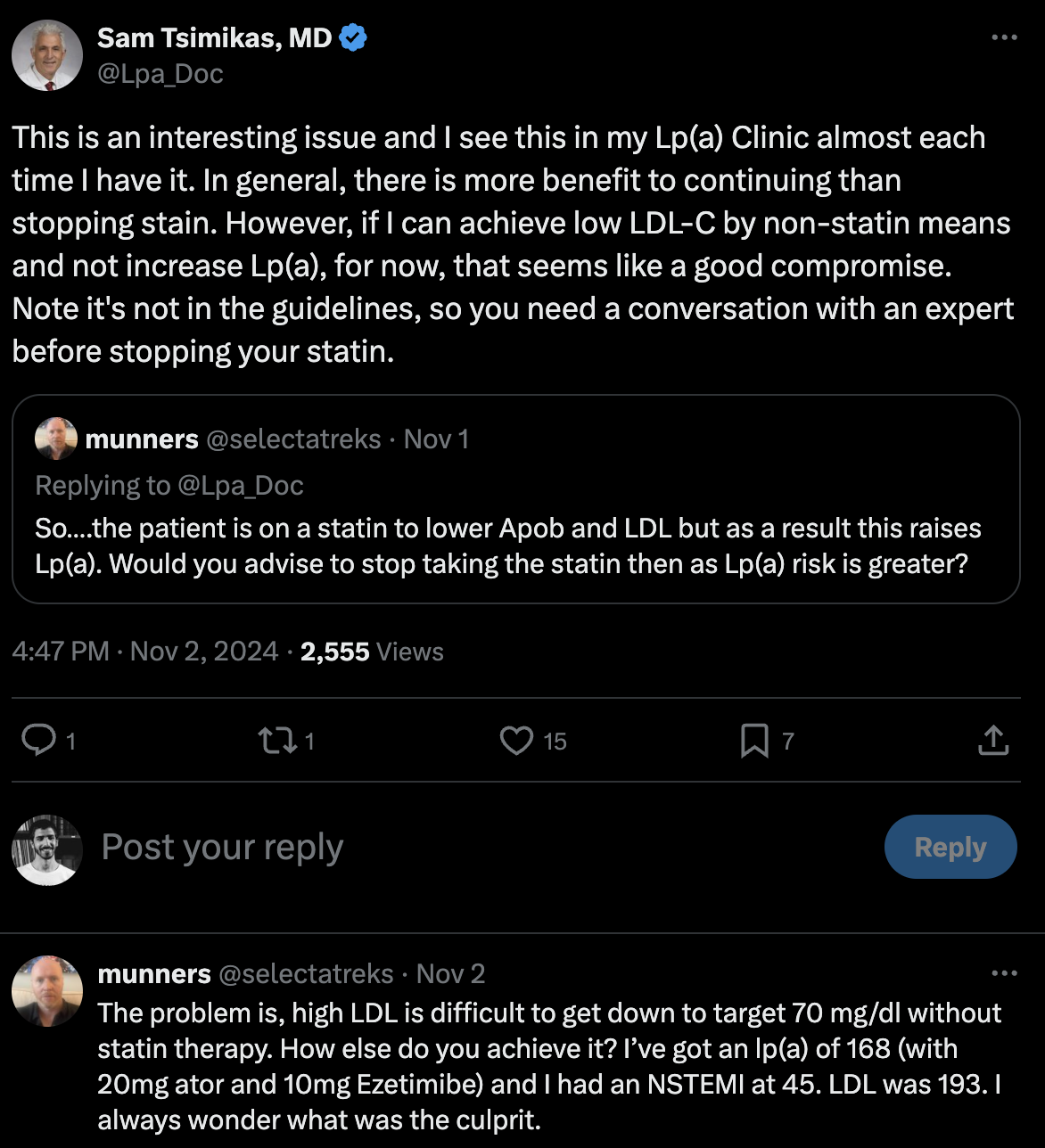
And yeah, it’s bad news. It probably means that people with high Lp(a) should try to reach their LDL-C target without a statin as statins can increase Lp(a) even more:
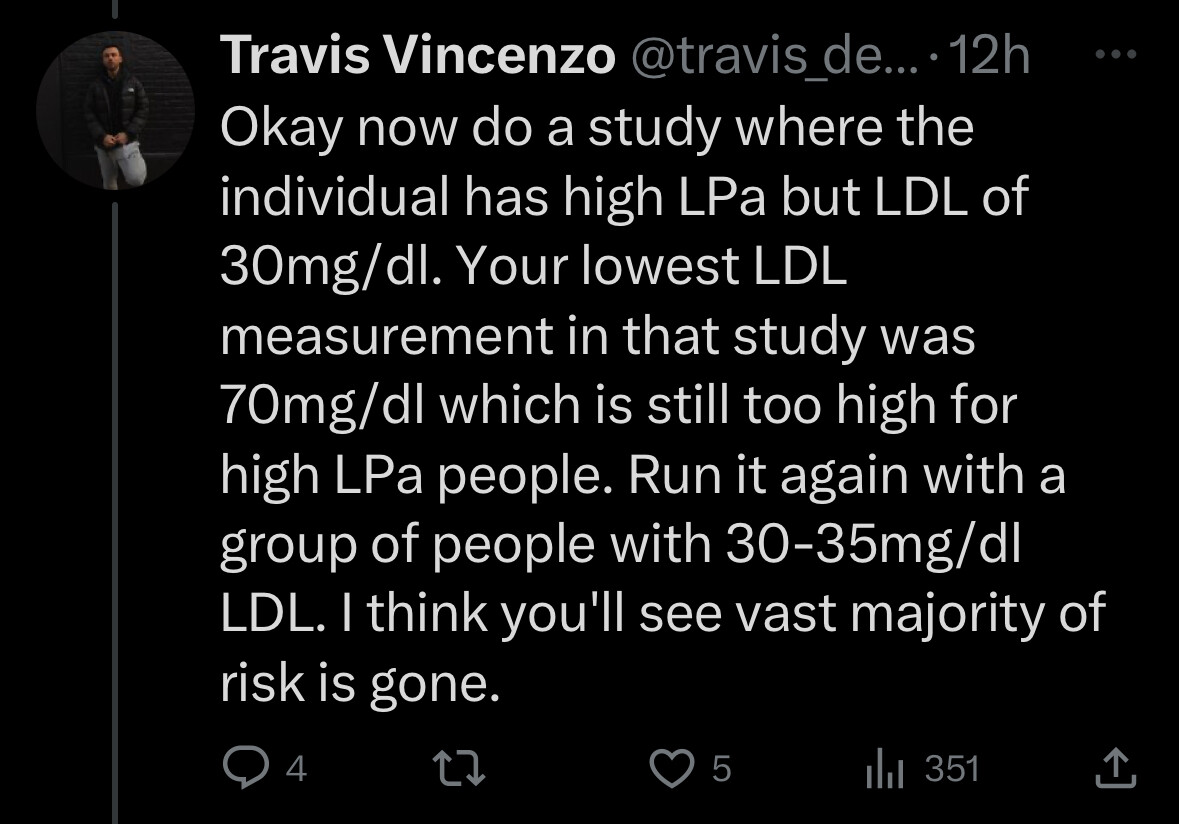
Sam Tsimikas’ answer to the suggestion to look at people with LDL-C ~ 30 mg/dL:
Lp(a)HORIZON (pelacarsen vs placebo) will read out in early 2025. It’s phase 3 so if positive, approval is possible in 2026? Same for obicetrapib. They both lower Lp(a) by about 60%. So the problem of elevated Lp(a) might be “solved” in a couple of years for people with Lp(a) around 100 mg/dL (to go below 50). Those with Lp(a) > 100 mg/dL might have to wait for olpasiran (phase 3 results in 2027) and lepodisaran (phase 3 results in 2029) that crush Lp(a) almost to zero.
6 Likes
adssx
#186
EICOSAPENTAENOIC ACID INHIBITS LIPOPROTEIN(A) OXIDATION DUE TO SCAVENGING MECHANISMS IN VITRO 2024
Elevated Lp(a) levels are an independent and causal risk factor for cardiovascular disease with limited treatments currently available. Oxidized Lp(a) stimulates foam cell formation, endothelial dysfunction and inflammation.
Lp(a)-enriched ApoB particles underwent time-dependent oxidation, reaching a peak oxidation value after 2 hours (27-fold, 0.45 ± 0.07 vs 12.60 ± 0.24, p <0.001) that were sustained through 4 hours. EPA significantly inhibited Lp(a) oxidation in a time-dependent manner through 3 hours. After 3 hours, EPA inhibited oxidation by 31% (8.04 ± 0.79 μM, p <0.001) while EA had no activity.
EPA inhibited oxidation of Lp(a)-enriched plasma in a time-dependent fashion consistent with a free radical scavenging mechanism. The potent antioxidant actions of EPA may contribute to reduced CV events in REDUCE-IT, including those subjects with elevated Lp(a).
Is the above clinically relevant?
5 Likes
Ulf
#187
I tried gemfibrozil and it did not lower my high lp(a).
Am researching the merits of the anecdotal reports of amla + lysine and Vit C + collagen reducing lp(a).
4 Likes
Ulf
#188
In vitro studies rarely prove to be clinically relevant.
FWIW, my big intake of EPA from >1 kilo of fat fish per week has done nothing for my lp(a).
4 Likes
adssx
#189
From what I understand the paper doesn’t claim Lp(a) lowering but lowering its oxidation so potentially making it less “harmful”. Could it explain the MACE reduction in REDUCE IT (pure EPA)?
2 Likes
Davin8r
#190
Have we talked about this paper before? It’s a meta analysis of CoQ10 and Lp(a) lowering. At first, the degree of lowering seem trivial, but in the fine print:
[CoQ10 supplementation led to a]…“numerically greater reduction in plasma Lp(a) concentrations in the subset of trials with baseline Lp(a) values ≥ 30 mg/dL (WMD: -11.72 mg/dL, 95% CI: -21.01, -2.42,
p=0.013) compared with the subset with baseline values < 30 mg/dL (WMD: -3.14 mg/dL, 95% CI:
-4.92, -1.35, p=0.001”
Also: “Subgroup analysis suggested that the impact of CoQ10 on plasma Lp(a) was greater at supplemental doses < 150 mg/day (WMD: -9.24 mg/dL, 95% CI: -15.19, -3.29, p = 0.002) compared with doses ≥ 150 mg/day (WMD: -2.75 mg/dL”
So I wonder what the average reduction would be in someone using both a low dose of CoQ10 and who had a higher baseline Lp(a)?
That 11.72 reduction is significantly higher when converted to modern units (nmol/L), this is roughly 12 x 2.5 = 30 nmol/l, right? Not huge, but definitely significant.
Add a daily baby aspirin to that to knock it down a little more (along with platelet inhibition).
CoQ_Lpa_Review.pdf (1.1 MB)
2 Likes
adssx
#191
It would be good to have more recent papers on the topic, but note CoQ10 also has a U-curve for glucose and blood pressure with an optimum around 100 mg/day: Coenzyme Q10 (CoQ10) U-shaped dose-response relation with blood glucose and blood pressure
Bryan Johnson takes 50 mg/day of ubiquinol (reduced Q10).
4 Likes