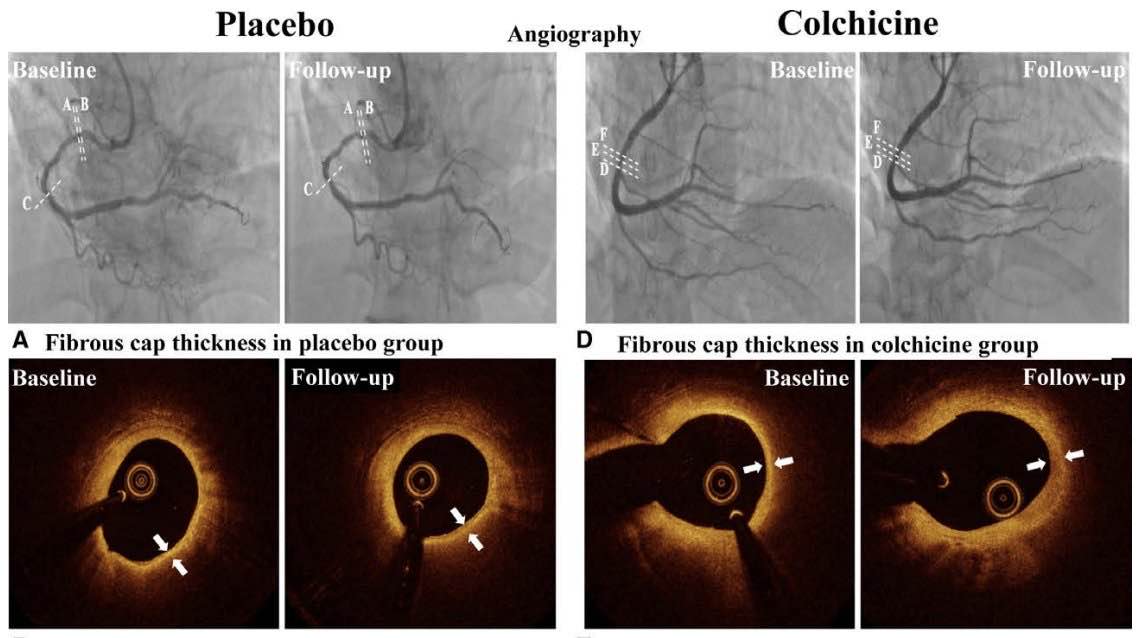
In this study, we first clarified the effects of colchicine on coronary plaque characterization by OCT and yielded the following findings: (1) plaque stabilization was improved under the anti-inflammatory treatment with colchicine in patients with ACS, as evidenced by a greater increase in FCT, a decrease in the lipid arc, and reduced macrophage infiltration in OCT; (2) colchicine significantly reduced the levels of IL-RA/IL-18/IL-6/hsCRP and MPO/AZU1.
Dyslipidemia and inflammation jointly contribute to atherothrombotic disease. In contemporary practice, lipid-lowering therapies such as statin, ezetimibe, or PCSK9i (proprotein convertase subtilisin/kexin-9 inhibitors) therapy are currently recommended in almost all patients with CHD to reduce cardiovascular event risk.24 Most guidelines for CHD have appropriately endorsed the concept that lower LDL-C is better worldwide. The plaque-stabilizing properties of lipid-lowering therapy have been evaluated by OCT in several studies.16,17 As shown in a recent study, residual inflammatory risk was more strongly associated with future cardiovascular events than residual cholesterol risk. However, it was unclear whether therapy targeting inflammatory risk could translate into favorable plaque modification in ACS. Herein, we indicated that OCT parameters including FCT, lipid arc, and macrophage infiltration were improved under colchicine therapy in patients with ACS, which provided the direct evidence that anti-inflammatory therapy could induce plaque stabilization. For subgroups analysis, patients with baseline LDL-C≤70 mg/dL could benefit more significantly from plaque stability, which further indicated that targeting residual inflammation risk could be beneficial in patients with CHD with well-controlled LDL-C.
In the present study, the percentage change of minimum FCT in the placebo group was greater than the HUYGENS and PACMAN-AMI studies.17,26 This difference is mainly related to the lower LDL-C control during the follow-up period in the placebo group (61.8 mg/ dL) compared with the HUYGENS (87.2 mg/dL) and PACMAN-AMI (74.4 mg/dL) studies (Table S4). The differences in population and risk profile might also result in the differences in the OCT parameter levels between this study and previous studies. Moreover, in this study, the percentage change of minimum FCT in colchicine group was also greater than the previous studies of evolocumab and alirocumab.17,26 **From the perspective of clinical end point, evolocumab and alirocumab reduced the risk of major adverse cardiovascular and cerebrovascular events by 15%.27,28 Colchicine reduced the risk of major adverse cardiovascular and cerebrovascular events by 23% in COLCOT.**8 Anti-inflammatory treatment with colchicine leads to a more significant reduction in the risk of major adverse cardiovascular and cerebrovascular events compared with the lipid-lowering treatment with PCSK9i, which is consistent with the more significant changes in minimum FCT caused by colchicine.
The favorable effects of colchicine on coronary plaque stability were found in the inhibition of inflammation. Recently, a few studies have explored several anti-inflammatory mechanisms potentially explaining the atheroprotective actions of colchicine including **the inhibition of neutrophil activation, neutrophil-platelet interactions, and NLRP3 inflammasome assembly by the interference with microtubule function.**11 The anti-inflammatory mechanism of colchicine seems to vary depending on the different hsCRP levels. hsCRP is the indicator of NLRP3/IL-1β/IL-6 axis activation. In the patients with CHD with hsCRP>2 mg/L, the anti- inflammatory effect of colchicine has primarily focused on the NLRP3/IL-1β/IL-6 pathway.13,29 During atherogenesis, activation of the NLRP3 inflammasome within plaque promotes the local generation of proinflammatory cytokines, which promote necrotic core formation by increasing cell death and accelerate fibrous cap thinning by degrading extracellular matrix macromolecules.30–32
Herein, the median of hsCRP level was 1.2 mg/L in the colchicine group, which was <2 mg/L. This was consistent with previous reports the hsCRP concentration had ethnic differences with especially lower levels in the East Asian populations.33 It was reported that the neutrophil signaling implied an advantageous role for proinflammatory activation in patients with atherosclerosis with hsCRP≤2 mg/L in addition to the NLRP3/IL-1β/IL-6 pathway.34 Neutrophil-driven proinflammatory responses could cause an inflammatory environment that promotes plaque destabilization and triggers thrombus formation.35 The LoDoCo2 sub-study indicated that neutrophil activation were obviously downregulated after colchicine treatment in the patients with CHD with hsCRP≤2 mg/L (median hsCRP level, 1.52 mg/L).36
In this study, we also found a significant reduction in neutrophil activation (MPO/AZU1) besides NLRP3 inflammasome activation (IL-1RA/IL-18/IL-6/ hsCRP) after colchicine treatment in patients with ACS. The correlation analysis between the changes in OCT parameters and inflammatory biomarkers further clarified this point of view. We showed that the changes in IL-6 and MPO were positively correlated with the percentage change in the average lipid arc after colchicine administration.,Collectively, the potential anti-inflammatory mechanisms of colchicine seemed to diverse, mainly targeting both neutrophil and NLRP3 inflammasome pathways. In addition, we found that the change of IL-6 was correlated with plaque stability. It indicated that IL-6 might be a suitable biomarker in vascular inflammation, as suggested by the subanalysis of CANTOS.
Taken together, the findings show that anti-inflammatory therapy is one of the most promising strategies for combating residual cardiovascular risk. Although the favorable effects of colchicine on ACS were recommended in current guidelines based on the COLCOT study,38 the mechanism remain ill-defined. The increased risk of recurrent atherothrombotic events is mainly attributable to the progression of nonculprit lesions in ACS.39,40 PCI is an important treatment for ACS, but plaque burden and unstability in the nonculprit lesion are significantly aggravated after PCI because of the stenting-triggered inflammation. Thin fibrous cap and macrophage infiltration are the important discriminators of the high-risk unstable plaque, which lead to the increased risk for recurrent adverse cardiac events after ACS.42,43
Our findings first revealed that colchicine favorably modified nonculprit plaque by increasing the FCT and alleviating macrophage infiltration through its anti-inflammatory effect, which provided the mechanistic rationale in favor of colchicine reducing recurrent atherothrombotic events in ACS, and were helpful for the interpretation of the COLCOT study. For culprit plaques, fibrous cap rupture and erosion are the 2 leading mechanisms that induce ACS, and the effect of colchicine on different culprit lesion phenotypes should be further explored. In addition, the strategy of drug-coated balloons would allow antiproliferative drug delivery to vulnerable plaques and medical therapy to be active in favoring plaque regression. The impact of oral colchicine therapy on 2 different PCI strategies (drug-coated balloons or drug-eluting stents) needs further exploration.
The proportion of unstable angina among patients with ACS was relatively high in this study compared with the typically observed rates in Europe.44 One possible reason was that the proportion of unstable angina among ACS was higher in China.45 Another possible cause was that certain patients with acute myocardial infarction could not tolerate prolonged OCT detection of all the 3 main epicardial coronary arteries. For patient safety reasons, these patients with acute myocardial infarction were not enrolled. In addition, some patients with acute myocardial infarction only underwent the revascularization of the culprit lesion during hospitalization, and they were excluded because of incomplete revascularization according to the inclusion criteria.