mccoy
#953
adssx, I think the cherry picking (discarding outliers or suspicious values), is acceptable when attempting to reach an objective conclusion and not just pushing an agenda.
2 Likes
adssx
#954
I agree. I just wanted to be clear for those reading us that for now there’s no definite answer as to whether ezetimibe + low or medium dose statin is better than high intensity statin alone in terms of outcome.
Thankfully, several ongoing trials are looking at this question: ClinicalTrials.gov
We’ll have to wait a few years to get the results though… In the meantime we have to rely on the above…
1 Like
A_User
#955
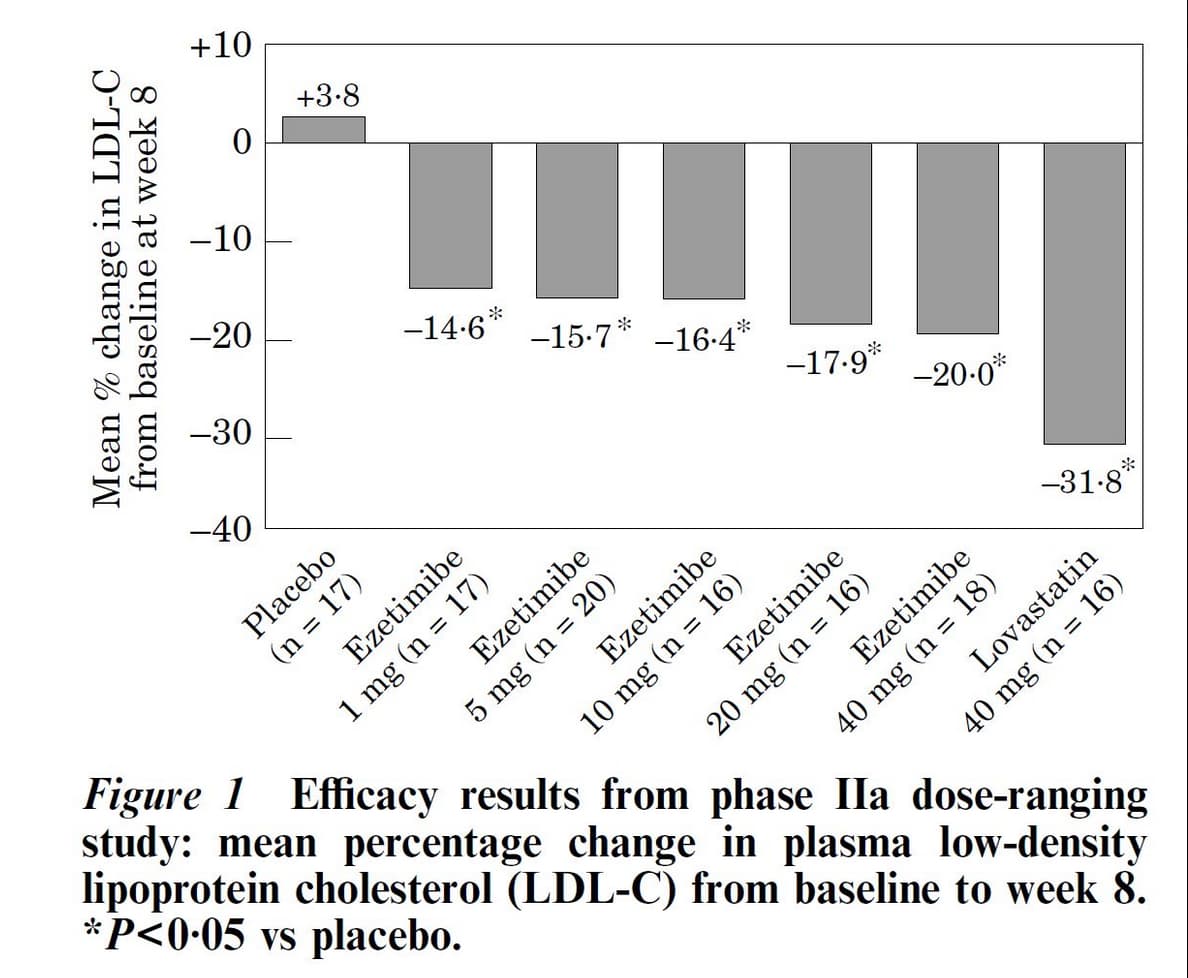
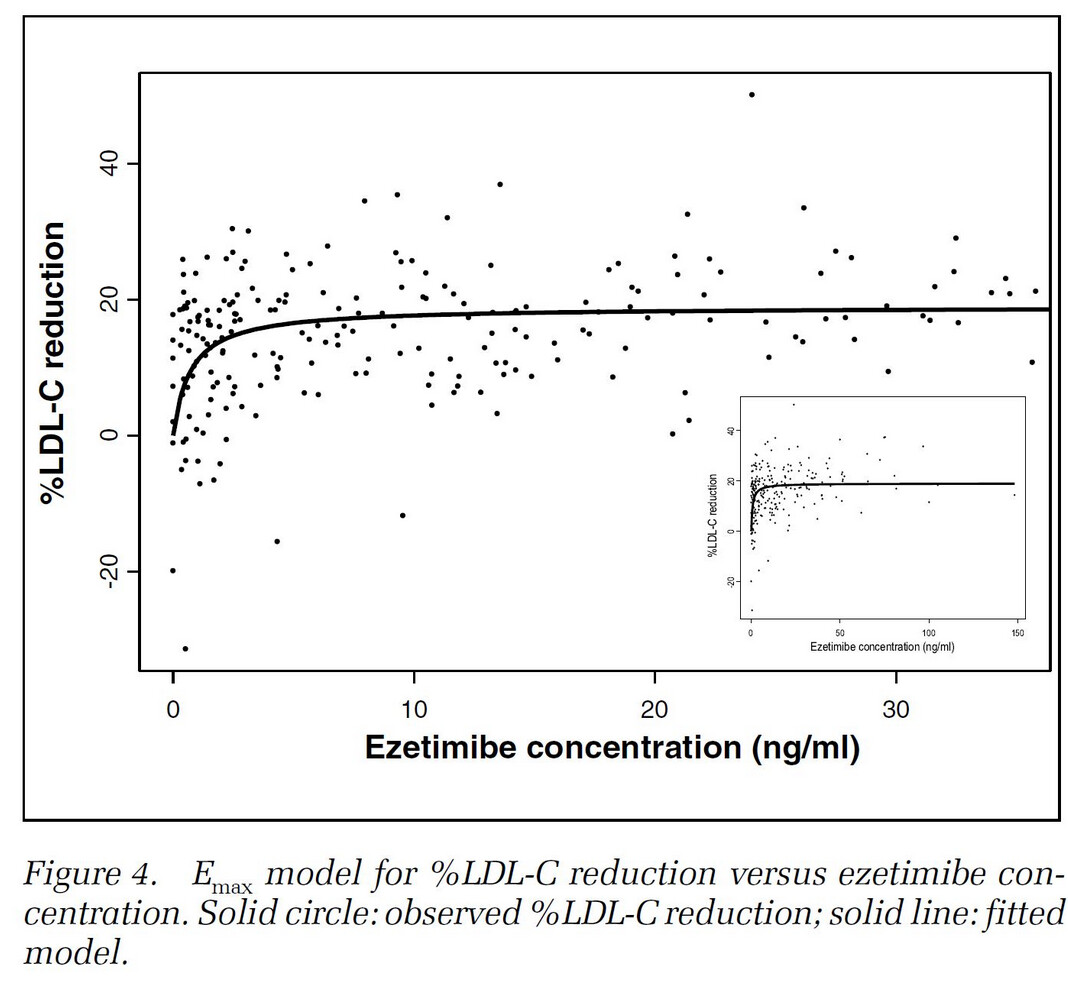
Effect on LDL up to 40 mg ezetimibe:
https://x.com/Drlipid/status/1823755001422078178
Atorvastatin is generally considered the first choice.
4 Likes
mccoy
#956
Yes, I’m just reading the details now and unfortunately the improvements in the combo with respect to simple statins are statistically significant but not that glamorous in average
LDL-C reduction (Mean Difference (MD) -5.05 mg/dL; 95 % CI [-9.02;-1.07]
Also, ApoB seems unaffected by the combo with respect to the control…
I wonder if there are in commerce reliable devices to check lipids with a finger prick and reactive strip, this would be the best strategy to ascertain on an individual basis the results.
adssx
#957
Yes tiny LDL difference but big difference in % of people who reached the 70 mg/dL target.
1 Like
Davin8r
#958
Note: thread title is “2019” but the study discussed below is brand new, published in Circulation 8/21/24
I thought this is worth cross posting. Attaching CVD through anti-inflammatory pathways using low dose colchicine appears to be a great option to decrease risk after maximally lowering ApoB. I’ve been on the fence, but this new study pushed me to go ahead and ask my PCP for colchicine Rx.
There is danger in extrapolating an effect of a medication in disease to individuals without disease. Trivial example: two patients with a life threatening bacterial infection - one of them is given a powerful antibiotic and survives, the other one dies. So a paper is written: survival advantage of Powerful Antibiotic. And then longevity fans all start taking Powerful Antibiotic and disaster results.
Drug extends life, has good effect in people with a given disease? I don’t have that disease, should I take it for my health/longevity? That’s the question. Why do I like ITP trials? Because they’re in healthy mice. Not like those studies where they use genetically messed up mice give them “SPECIAL DRUG” to compensate for that particular mess, then declare “life extending benefits of special drug” and we all immediately take it even though we don’t have the mess condition. Here’s my longevity recommendation: pillow taped around the body - my proof, in my experiment, I smashed mice with a hammer, but the ones wrapped in pillows had a survival advantage. Ergo, we should all wrap ourselves in pillows. But ITP studies are still in mice - people, who knows.
Does this drug advantage healthy people, based on studies in sick people?
2 Likes
Davin8r
#960
Are you talking about colchicine? I doubt such a study will ever be done in humans, but for those of us at high risk due to genetics (Lp(a), FH, etc) this approach could be a real breakthrough. I’m not suggesting they put colchicine in the water supply.
1 Like
mccoy
#961
I really find it hard to believe… at 1 mg, 1/10th the minimum commercial dosage, the effect is just about the same than at 10 mg. I wish there were a way to split the pill in tenths.
Why?
adssx
#962
The half life is 22h so you can split in two and take it every other day. It might be doable to split in 3, but the ezetimibe 10 mg pill is already so small…
1 Like
mccoy
#963
I’m thinking about something similar with one pill of Rosumibe 5/10 and one pill of Rosuvastatin which has a half life of 19 hrs.
-Day one: 1/4 pill of rosumibe 5/10; Provides Ezetimibe= 2.5 mg, Rosuvastatin 1.25 mg
-Day two: 1/4 pill of Rosuvastatin, provides 1.25 mg
-Day three: 1/4 pill of rosumibe 5/10; Provides Ezetimibe= 2.5 mg, Rosuvastatin 1.25 mg
-Day four: 1/4 pill of Rosuvastatin, provides 1.25 mg
-…same as above
In such a way, I could have an average daily dose of 1.25 mg Ezetimibe and 1.25 mg Rosuvastatin, which sounds pretty optimal.
The drawback would be the pill splitting and conservation.
I would be open to alternatives.
FYI, here’s my results before and after taking BA (140 mg) + Ezetemibe (10 mg) + Atorvastatin (5 mg)
You can see LDL went from 122 to 48 and ApoB went from 102 to 48.
8 Likes
mccoy
#965
The results are impressive, back to the panel of a 10-years boy perhaps and without even using PCSK9-inhibitors.
What governed your choice of Atorvastatin?
1 Like
I tried Rosuvastatin first, but I was intolerant. Atorvastatin worked for me. Without Atorvastatin,my LDL and ApoB were 68. Atorvastatin makes a significant difference.
Although my LDL was 67 before Rapamycin, it’s nice to see that this combination therapy reduced my cholesterol below pre-Rapamycin levels.
3 Likes
adssx
#967
I think atorvastatin and rosuvastatin are the most potent statins and the only ones to have shown all-cause mortality reduction in populations with “normal” cholesterol (JUPITER and ASCOT trials?). (@A_User is that correct?) So they’re considered the best choices to start. Some people are intolerant to one but not the other. And rosuvastatin has a higher risk of new onset diabetes vs atorvastatin. See also this discussion: Rosuvastatin versus atorvastatin treatment in adults with coronary artery disease: secondary analysis of the randomised LODESTAR trial (2023)
4 Likes
adssx
#968
You could just start with 1/4 of the combo pill every other day and see if well tolerated but not enough to reach your target after 3 months then you could move to 1/4 every day. It’s more manageable than alternating every other day between two pills. (If 1/4 every day still not enough you can add double to 1/2 every day or add bempedoic acid.)
2 Likes
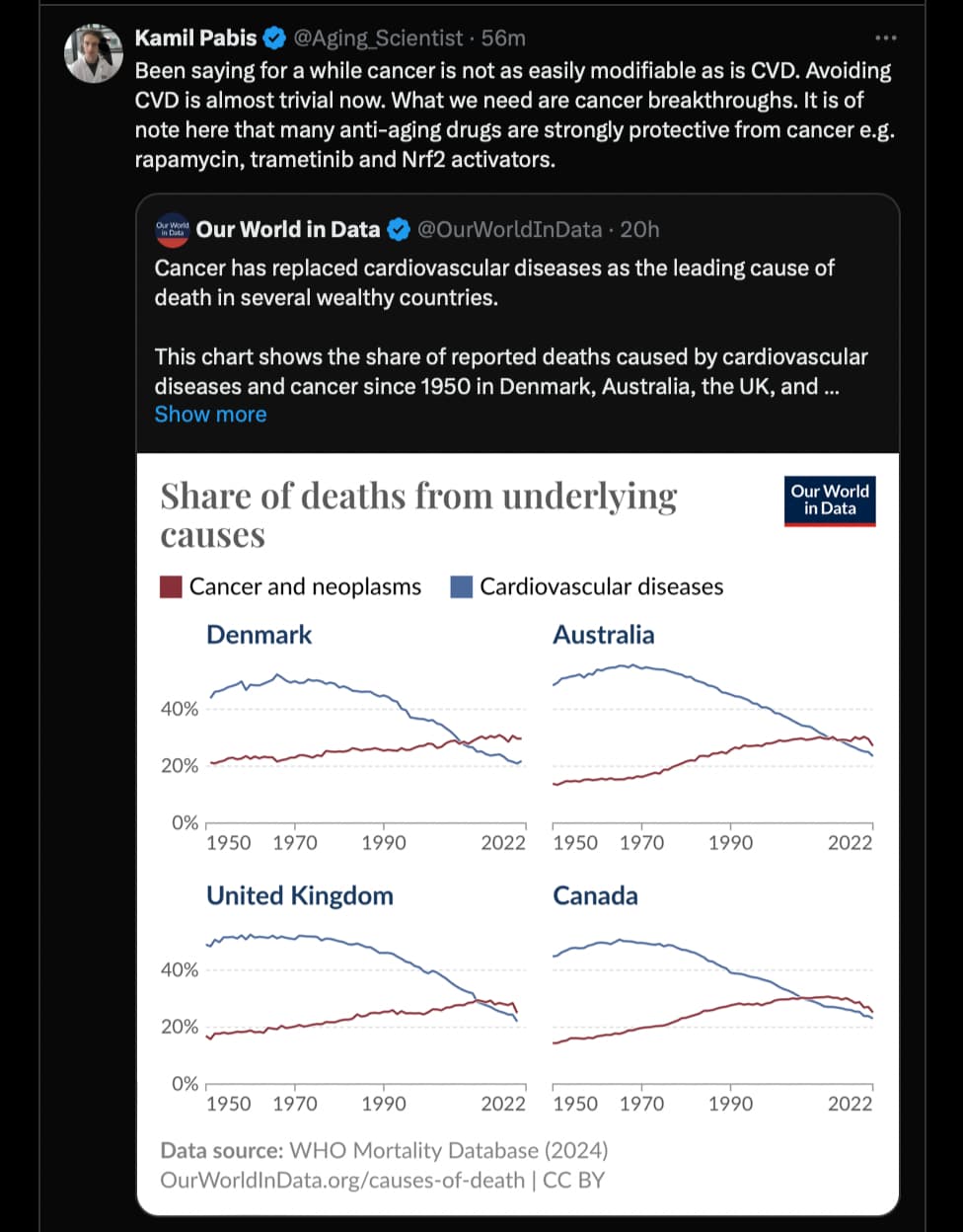
So, the argument this longevity researcher is making is that now that the Cardiovascular disease problem is “solved” (via early use of statins and other lipid lowering therapies - if used early enough) we should be focusing on cancer…
Source: x.com
2 Likes
There is plenty you can do about skin and prostate cancer already, but as for the rest, I’m not sure what can be done other than immune therapies. Even mice eventually succumb to cancer despite given multiple treatments at once.
1 Like
A_User
#971
I don’t know, I think all statins most likely improve all-cause mortality, and so do I think for all of the other lipid lowering treatments unless they’re banned drugs. Atorvastatin is preferred over rousvastatin according to the data IMO because of the diabetes risk difference. It’s also studied in the largest clinical trial ever done in older adults to see if it can reduce dementia risk.
So probably doesn’t matter that much. People who are APOE4 carriers or those with Alzheimer’s family history should probably consider measuring serum desmosterol levels to not crush synthesis too much. If they can’t do that lower dose statins and/or other treatments might be a good idea.
Also, to be honest, a small decrease in LDL from the mean has a massive effect if it’s lifelong, look at the PCSK9 loss-of-function studies.
2 Likes
I think the chances are that you are right in that statins direct acetyl-CoA away from cholesterol. I am not so sure mechanistically about bempedoic acid, but I am not worried about that.
1 Like