Great question!
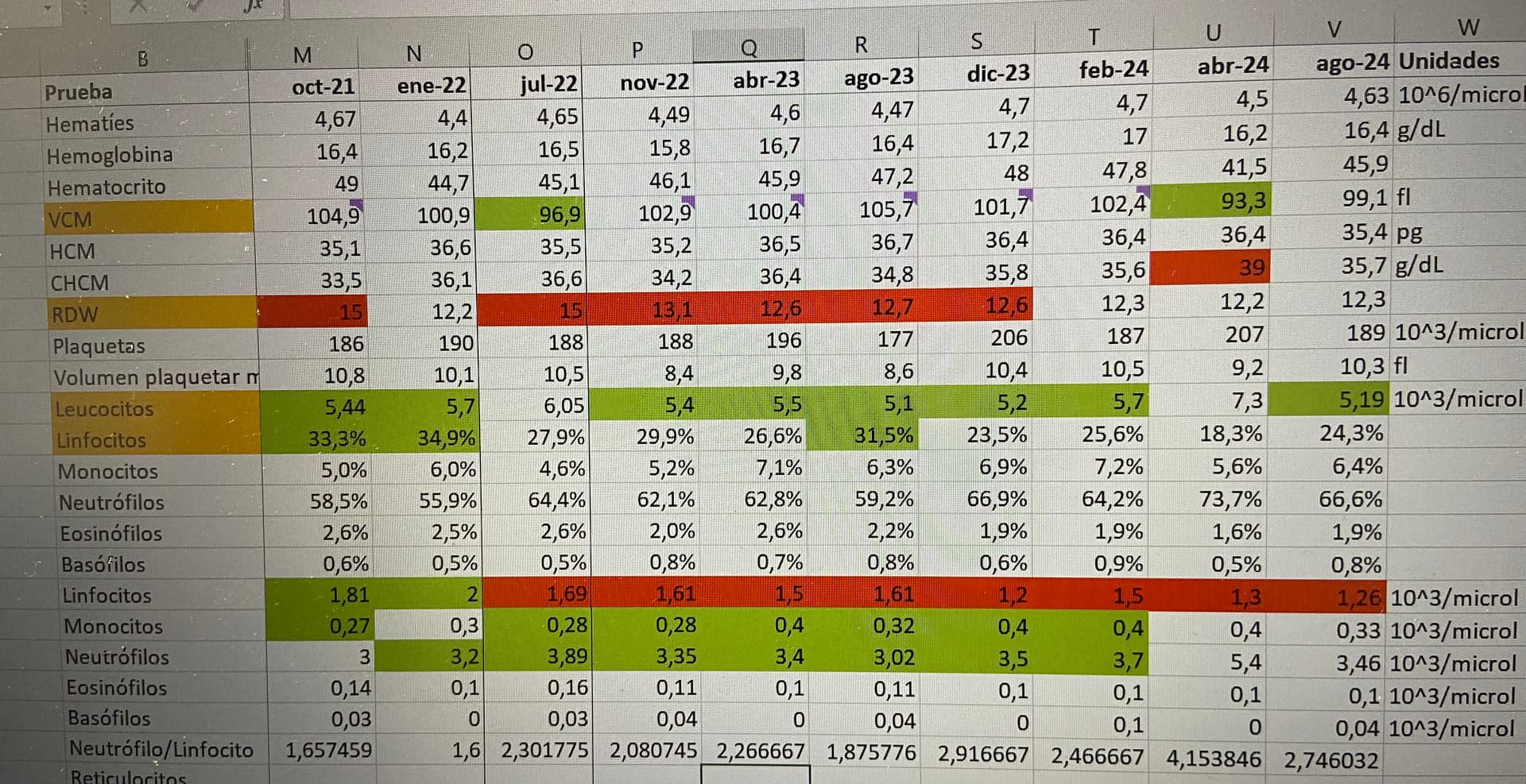
A red flag on anyone’s lab work is a high folate and a high homocysteine. This means, in general, folate isn’t getting utilized, which also indicates poor DNA methylation. The common situation is the folate >upper limit of normal.
My wife is a great example of this, homocysteine almost 30 and Folate>24. B12 normal. Pyridoxine (B6) also plays into high homocysteine, but this wasn’t going to be deficient.
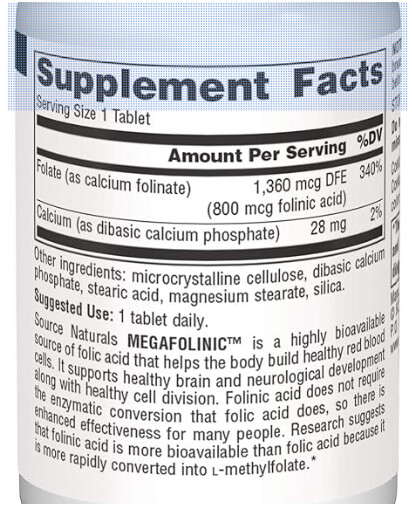
We went with folinic acid 800 mcg/day, a month later, homocysteine 9.
In this situation folinic acid requires no transport receptor to get into the cell, whereas MTHF does require a receptor. There can either be a defective receptor or an antibody to the receptor. Either way, bypassing this need for a specific way to transport folate into cells is the strategy with folinic acid.
It’s not even on the list of things to do for primary care physicians or cardiologists - yet, these patients have worse health outcomes. Here is what vera-health.ai says on health risks of high homocysteine:
Elevated homocysteine levels, known as hyperhomocysteinemia, are associated with several health risks, particularly affecting cardiovascular and renal health. High homocysteine is a recognized risk factor for cardiovascular diseases, including coronary artery disease, stroke, and acute coronary syndrome (ACS). Studies indicate that elevated homocysteine can lead to major adverse cardiovascular events (MACE) and increased all-cause mortality in ACS patients 1. This relationship may be due to homocysteine’s role in endothelial dysfunction, impairing nitric oxide production and contributing to coronary microvascular endothelial dysfunction (CMED) 2.
Elevated homocysteine levels are also linked to an increased risk of thrombus formation in patients with atrial fibrillation (AF), even among those with a low CHA2DS2-VASc score. Higher homocysteine levels correlate with a significantly increased prevalence of left atrial/left atrial appendage thrombus, suggesting a potential predictive role in thromboembolism 1.
In terms of renal health, homocysteine is associated with renal function decline, particularly in hypertensive patients. It correlates with decreased estimated glomerular filtration rate (eGFR), indicating its potential role in chronic kidney disease (CKD) progression 1. Elevated homocysteine is linked to metabolic syndrome and cardiovascular events in hypertensive patients, suggesting its contribution to cerebrovascular diseases 7.
Additionally, homocysteine may influence mental health, as elevated levels have been associated with major psychiatric disorders such as schizophrenia and bipolar disorder I, though not conclusively with depression 4.
Nutritional deficiencies, particularly in folic acid and vitamin B12, can exacerbate hyperhomocysteinemia. Supplementation with these vitamins can help reduce homocysteine levels, potentially mitigating some of the associated risks 5.
In summary, elevated homocysteine levels are associated with increased risks of cardiovascular diseases, thrombus formation, renal function decline, and certain psychiatric disorders. Addressing elevated homocysteine through lifestyle changes and appropriate supplementation may help reduce these health risks.