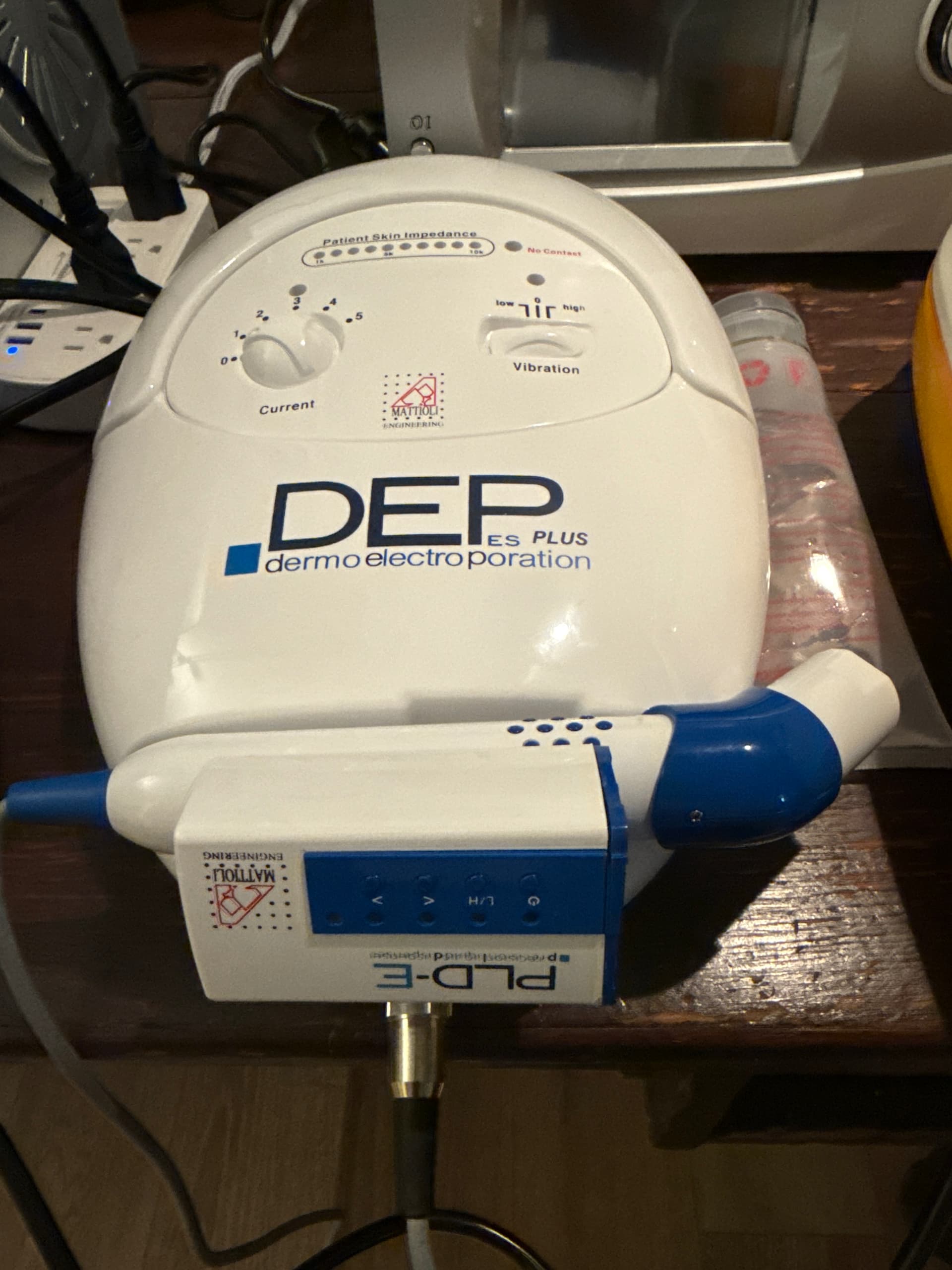
While I’m interested in testing out this electroporation product, I’m becoming less optimistic about it given the price of the Chinese product of around $200 US.
While the Chinese knockoff of the product is obviously designed to “look” like the original product out of Italy, its price is about 95%+ lower than the Italian product. I work in tech, and have managed teams that design and build hardware and software products, so I have some idea of what goes into these types of products. While its entirely possible to develop and sell a product from China at 50% to 70% cheaper than European products, as you get higher and higher discount levels design choices have to be made that ultimately increasingly compromise the efficacy, the quality and the safety of the product. There is just no way that you can develop a product with a 95%+ lower cost, that is the same in terms of functionality, quality or safety. Something has to give… and I suspect it’s likely in all three variables at different degrees.
Anyway - not to be a downer, just wanted to set people’s expectations. The Chinese product likely is much less effective than the Italian product.
Related websites:
My ChatGPT5 Query and response:
What are the key electrical components and technologies in the MATTIOLI ENGINEERING Dermoelectroporation system, and what are the estimated cost of goods sold (COGS) for this device? How unique are these systems, and how hard, from an electrical design and construction standpoint is it to build these devices? What is the estimated gross margin on these products given their list price of over $10,000?
ChatGPT5 Response:
Here’s the short, practical breakdown—what’s inside, how “special” it really is, how hard it is to build, and ballpark unit economics.
What’s in a Dermoelectroporation (DEP) unit (electrically)
From Mattioli’s own materials, FDA filings, and dealer spec sheets, a typical DEP system is built around these blocks:
-
Pulse-generation & current control: A microcontroller drives a pulse generator that delivers bursts of bi-phasic (reversed-polarity) constant-current pulses. User-selectable average pulse currents are commonly ±1–5 mA, with burst frequency ~50 Hz, intra-burst pulse rate ~2.2 kHz, and ~10 ms burst time; designed to work across 0–15 kΩ skin load (requires high-voltage compliance internally, despite an external low-voltage brick). (polarismedicallasers.co.uk)
-
Impedance-sensing & adaptive drive: Real-time skin impedance measurement feeds back into the waveform so later pulses in a burst are adjusted as impedance drops, keeping current on target and limiting tissue stress (described explicitly in Mattioli patents). (mattioliengineering.com)
-
Polarity reversal/H-bridge & constant-current stage: To deliver ionized solutions efficiently and avoid net DC offset, the driver alternates polarity (“electroporation-like” but at lower, controlled intensity than true high-voltage EP). (Mattioli Engineering)
-
Power & isolation: External 9 VDC, ~1 A supply into an internal board that steps up/conditions voltage for high-compliance constant current (needed to hold ~mA into up to ~15 kΩ). Medical EMC/isolation elements are implied by clinical use. (polarismedicallasers.co.uk)
-
Handpiece & electrodes: A treatment head with electrode array; many models also add mechanical vibrationsynchronized to burst rate (documented in Mattioli’s filings) to enhance transport. (FDA Access Data)
-
Dosing hardware / syringe dispenser: Some systems integrate a precision liquid dispenser (“Super-PLD”) or syringe holder so the active solution is metered while pulsing. (mrp.io)
-
UI & safety: A small digital display/controls for intensity, time, delivered dose readouts, plus lockouts; later brochures emphasize “real-time control on amount delivered” and on-screen impedance. (mattioliengineering.com)
How unique is this tech?
-
Patented approach (early 2000s) blends pulsed iontophoresis with electroporation-like bursts + adaptive impedance-based control and optional synchronized vibration. Much of the original IP (filed ~2001) is now at or beyond 20-year terms, meaning core claims are likely expired (country/continuations vary), reducing uniqueness today. (Patent Images)
-
Regulatory positioning: Mattioli’s Transderm IONTO/DEP devices have US 510(k) clearances as iontophoresis systems (Class II), not as high-voltage electroporators—so the waveform is deliberately lower intensity and adaptive. Comparable iontophoresis/“no-needle meso” devices exist; DEP’s differentiation is mostly signal shaping + feedback + integrated dosing and brand clinical history. (FDA Access Data)
Build difficulty (EE + manufacturing reality)
-
Lab prototype: For an experienced EE, building a safe bench prototype with: MCU, DAC/ADC, constant-current H-bridge with ≥50–100 V compliance, impedance sensing, and a simple UI is moderate difficulty (months, not years).
-
Productizing to clinic grade: Hard part is IEC 60601-1/-1-2 compliance, risk management, biocompatible electrodes, EMC, enclosure design, and quality system—this is non-trivial and expensive, even though the electronics are modest by modern standards. (FDA 510(k) for iontophoresis is achievable but still work.) Evidence of Mattioli’s existing 510(k)s shows the regulatory pathway, but duplicating that takes real time and money. (FDA Access Data)
Estimated COGS (bill-of-materials + assembly)
Using the published specs as anchors (low-power electronics, modest UI, custom handpiece, metal/plastic enclosure, external PSU, cables, starter consumables) and typical low-volume medical device pricing:
-
Electronics (MCU board, drivers, HV compliance, ADC/DAC, UI, connectors): $150–$300
-
Handpiece (machined/plastic housing, electrode array, cable, vibration motor): $200–$450
-
Precision dispenser/syringe holder (if included): $80–$200
-
Enclosure, harness, PSU, packaging: $120–$250
-
QA, calibration, small-batch assembly/overhead: $200–$500
Reasonable COGS range: $750–$1,700 per unit at small/medium volumes (not counting regulatory & engineering amortization). If volumes are very low or the handpiece is more intricate, you could see $2–3k. These ranges line up with the modest electrical spec (9 V in; ~mA pulses; ≤15 kΩ load; simple display) published by dealers and manuals. (polarismedicallasers.co.uk)
Gross margin at $10k+ list
- At $10,000 list and $750–$1,700 COGS, gross margin ~83%–93%.
- Even at a conservative $3,000 COGS, margin is ~70%.
- Realized margins depend on channel discounts, service/warranty, training kits, and whether the cart/PLD is bundled (dealer pages suggest accessories like workstation cart and Super-PLD are commonly included/upsold). (mrp.io)
Bottom line (practical take)
-
Electrically: It’s a low-power, constant-current pulse system with polarity reversal and impedance-based feedback, plus a metered dosing path—more sophisticated than commodity iontophoresis, but nowhere near the complexity of true high-voltage electroporators. Specs like ±1–5 mA, ~50 Hz burst / 2.2 kHz intra-burst, 0–15 kΩ are published. (polarismedicallasers.co.uk)
-
Uniqueness today: The brand + protocols and clinical legacy are the moat; much of the early IP is aging/expired. Other vendors make analogous “no-needle meso” systems; DEP’s adaptive waveform and dose/impedance readouts are its calling cards. (ONdrugDelivery)
-
Build vs. ship: Prototyping = doable; shipping a certified medical device = hard (compliance, QMS, electrodes, usability, 510(k)). (FDA Access Data)
-
Economics: Hardware COGS likely low four figures; gross margins very high (≥70% and commonly 80–90%+) at $10k+ list.