mccoy
#1
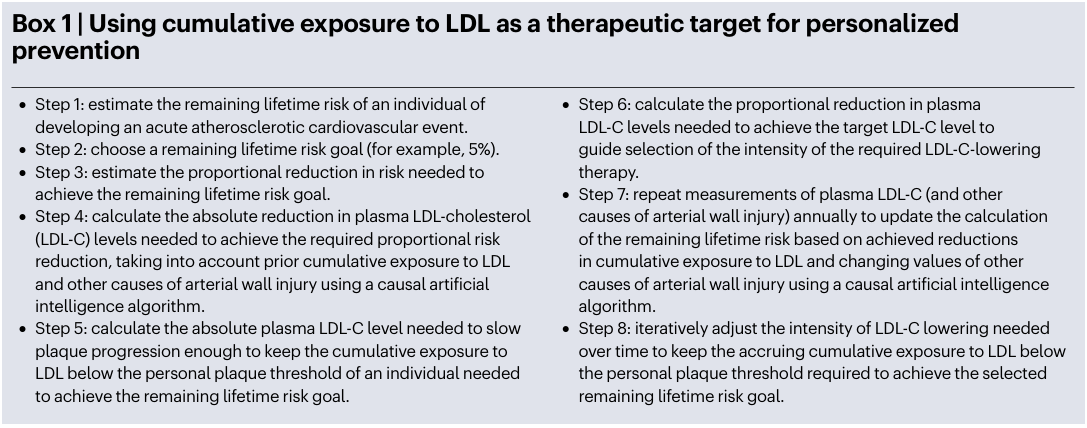
I opened this thread to exchange ideas about the practical procedure outlined in the object article, suggested by Dr. Lipid, posted by admin in the other general thread. A separate thread may help in keeping the discussion focused, plus I’m busy and need time to elaborate.
The authors basically propose the use of cumulative exposure as a risk index. Cumulative exposure is already the reference in many fields, such as lifetime exposure to air contaminants (silica, asbestos and so on).
5 Likes
mccoy
#2
Cumulative exposure to LDL-C is often expressed in units of
‘cholesterol–years’ or ‘LDL-C–years’, which are analogous to the frame-
work used in assessing the accumulative deleterious effects caused by
exposure to tobacco (‘pack–years’)88–92. However, these terms empha-
size the ‘cholesterol’ content carried by LDL rather than the concentra-
tion of atherogenic lipoproteins. Given that Mendelian randomization
studies clearly demonstrate that the cumulative number of LDL and
other APOB-containing lipoproteins that become trapped within the
artery wall over time determines the lifetime risk of having an ASCVD
event (and not the cholesterol content carried by those lipoproteins)73,
a more appropriate term might be ‘plaque–years’ of LDL (measured
in millimoles per litre or milligrams per decilitre). The term plaque–
years more accurately communicates that the rationale for measuring
cumulative exposure to LDL is to estimate the size of the accumulated
plaque burden and that the motivation for lowering LDL-C to reduce
cumulative exposure to LDL is to prevent atherosclerotic events by
reducing the size of the accumulated plaque burden.
This model is the same as those used in estimating lifetime cumulative risk in exposure to air contaminants like tobacco, asbestos, silica…
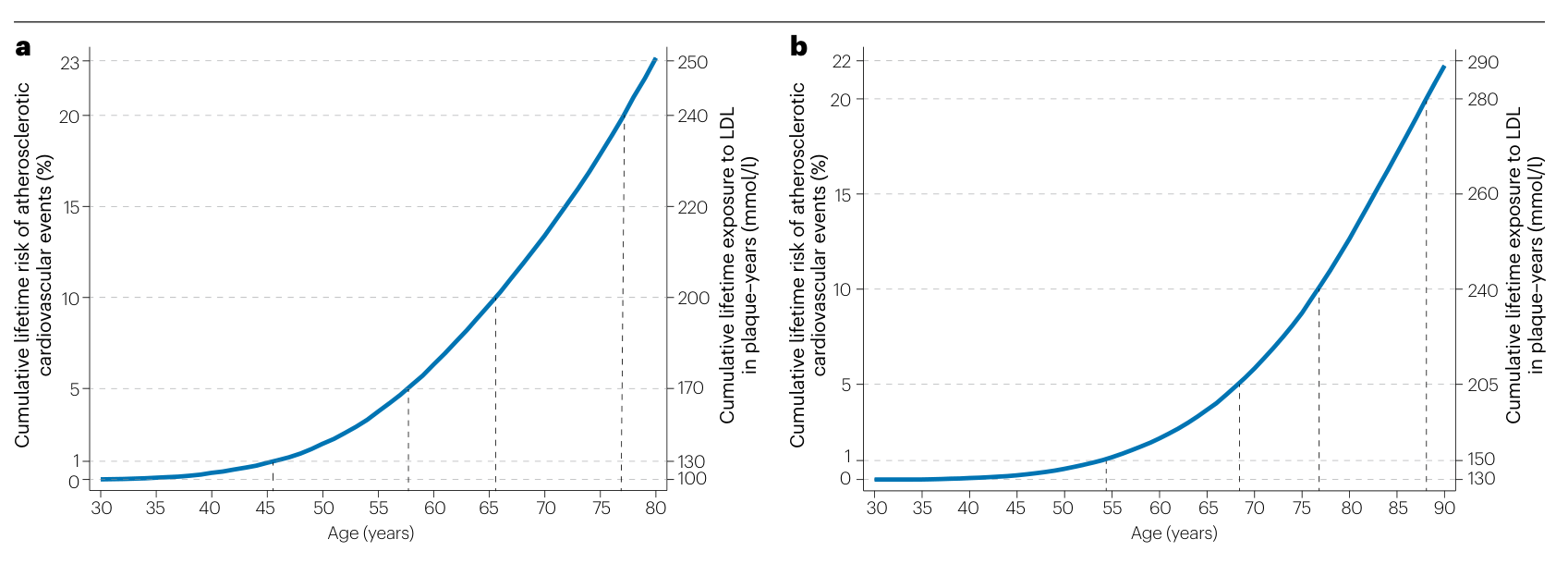
Among men
with average LDL-C levels and a typical LDL-C trajectory, the cumulative
lifetime risk of ASCVD events reaches 1% after 130 plaque–years (mmol/l)
of cumulative exposure and 10% after 200 plaque–years (mmol/l) (Fig. 3).
Among women, lifetime risk reaches 1% after 150 plaque–years (mmol/l)
of cumulative exposure and 10% after 240 plaque–years (mmol/l). The
apparent sex-specific differences in the cumulative LDL exposure thresh-
olds at which cardiovascular events occur could be explained, at least in
part, by the observation that oestrogen reduces the transcytosis of LDL
particles into the artery wall109,110. As a result, fewer LDL particles will be
trapped in the artery walls of women than in those of men with the same
LDL-C levels in the first ~50 years before the onset of menopause, which
translates to lower plaque burden and atherosclerotic risk.
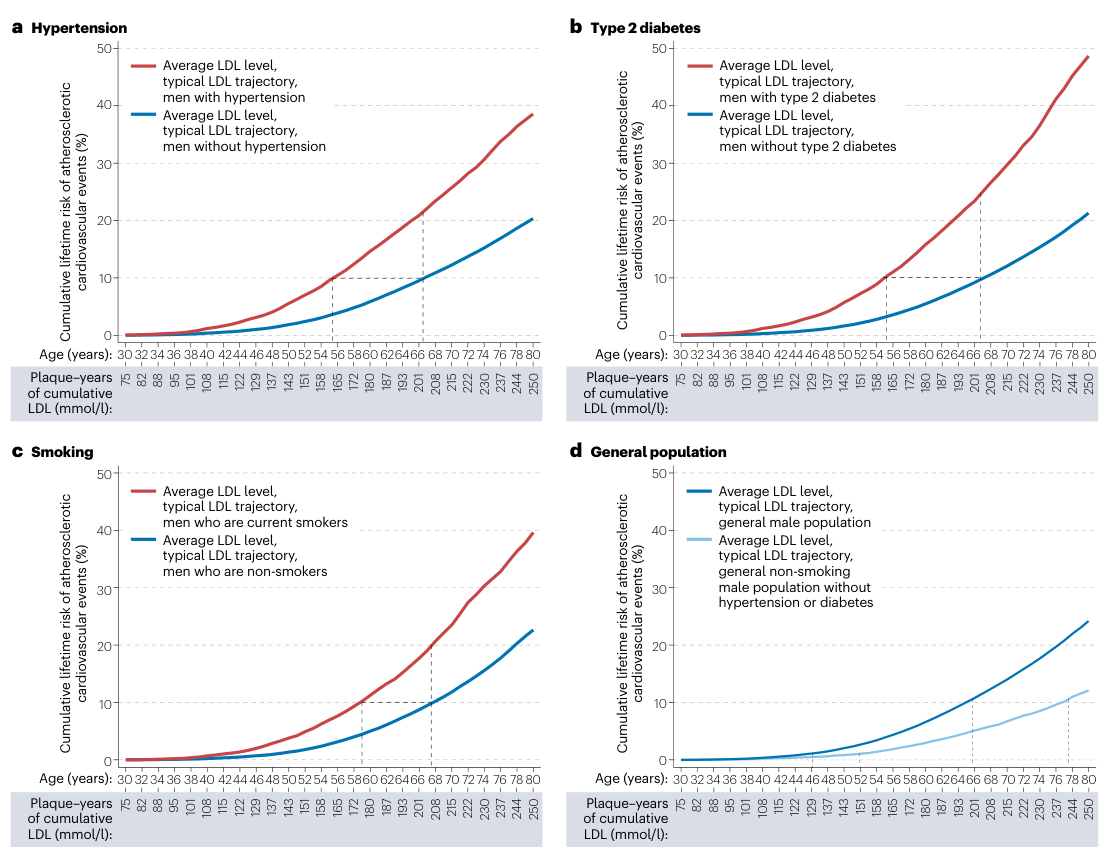
The authors start their reasonings from the temporal evolution of LDL-C concentrations in both genders. Of course this is an average across all population and we may estimate, based on these data and data collected on ourselves, our personal temporal evolution and from this our cumulative exposure at present age

A quick comment on the above graph: after age 40 in men LDL-C levels plateau at about 140 mg/dL (3.6 mmol/lt), it’s a pretty high value for health conscious individuals, who probably have an average plateau around 90-100 mg/dL or 2.3-2.6 mmol/lt (but this consideration is based upon my own values). The plateau value may vary of course across different populations, I noticed that values at age 21 in the table probably do not reflect average values in Italy, which seem to be about 0.5 mmol/lt less.
1 Like
I’m not sure what actionable items can be done in regards to this information other than lower your ApoB and LDL as much as possible.
Yet, even if you do lower LDL and ApoB, there is still some circulating in your blood therefore there’s always risk? Or is there a low level where plaque is impossible to form even with LDL present in the blood?
1 Like
mccoy
#4
DeStrider, and others, sorry I didn’t specify it clearly but the above was only the beginning, I think there are actionable items but I need some time to pinpoint the exact procedure, I’ll also try to apply it to my individual case and anyways I’ll go on posting interesting excerpts of the article.
2 Likes
Here is what Dr Twyman says to do;
-
Stop damaging the Glycocalyx (the protective barrier to the lining of arteries)
-
Stop making so many ApoB particles
-
Make more receptors to remove more ApoB particles
-
Lower reabsorption and absorption of cholesterol from food in gut
-
Damage to glycocalx
- Causes: high oxidative stress (mitochondrial dysfunction), inflammation from any source: gut related, infection (COVID), smoking, high insulin, high glucose
- Signs: high BP, erectile dysfunction
Blood markers review
- Homocysteine <10
- GGT high means low glutathione (high oxidative stress)
- Uric acid. High means poor metabolism. A marker of gout but also damaging to glycocalyx
7 Likes
mccoy
#6
The article does provide cumulative risk curves in the general population and in the presence of the main 3 aggravating factors: hypertension, smoking and diabetes. It does not provide a graph with the additive effect of the three, but it is clear it must be terribly higher.
1 Like
mccoy
#7
OK, that’s the first actionable thing we can do, it is useful to estimate where we are on the cumulative risk curve, whether we need a pharmacological intervention and which one(s), what will be the estimated outcome of an (estimated) decrease in LDL-C reduction.
- Estimate our own cumulative lifetime exposure. It is not easy especially so for those of us who don’t have an history of measurements except in the more recent times. I estimated my own lifetime risk by reasoning about what are my more recent values, what they might have been in the past, considering the shape of the reported curve of LDL-C increase for the general population.We may even build an optimistic and a pessimistic scenario and analyze both of em
- comparing our individual estimate (which among the younger ones may even be a close approximation) to the risk curve present in the article (I’ll post it later).
- build model for the future based on an expected reduction of LDL-c after personalized interventions.
For example, my optimistic cumulative lifetime exposure at 64 is 131 plaque-years (mmol/lt), which sits precisely upon the 1% lifetime risk of atherosclerotic CV events. These thresholds are visible in the following figure and are also provided in the text I pasted a few posts Above:
-1% cumulative risk= 130 plaque-years (mmol/lt) and 150 for women
-10% cumulative risk= 200 plaque-years (mmol/lt) and 240 for women
Men on LHS, women on RHS
2 Likes
mccoy
#8
What is the suggested threshold? I would say as low as possible of course and anyway it should be not much above the blue curves in the above graphs, which are relevant to the pessimistic, in my own view, data published in the article and whose source should be indagated.
The preliminary conclusion in my case is that my risk might be viewed as pretty low, so if I desire that it keeps so until age 100 (I’ll have to do simulations about that) I’ll have to adopt pharmaceutical intervention of a moderate extent probably.
This procedure is of course extendable to everyone
Bicep
#9
There are supplements specific for the glycocalyx, (I almost tried one but they’re expensive) did he recommend any of them?
1 Like
Here is what I put in the show notes from my interview with Dr Twyman:
- Supplements to consider
- Vit k2 - keep calcium in bone not arteries
- Garlic - support glyocalix health
- Berberine — increase LDL receptors (like a weak pcsk9)
- Bergomot - lower LDL production (like a weak statin)
- Ezetimibe (not supplement) — reabsorption of cholesterol
- Aspirin (81 mg) - complicated. Had an event? Aspirin for life. No event yet? Higher CAC? Aspirin. Unless high risk of bleeding.
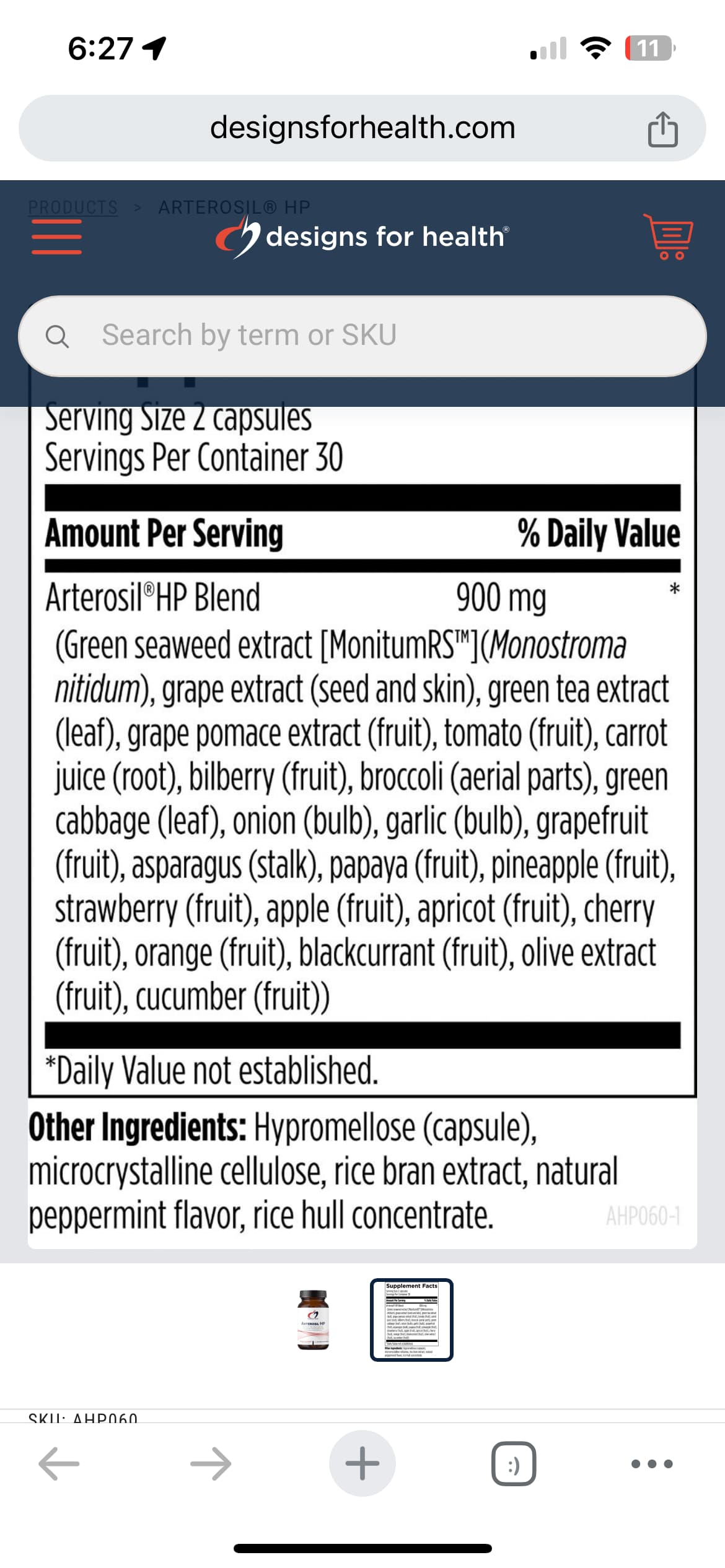
He sells Arterosil HP (I have it on my Fullscript site cheaper)
For myself I act as though everything that lowers inflammation is good for glycocalix:
-
exercise (not too much too soon, sufficient recovery, etc)
-
gut health
-
low AGEs
-
healthy blood sugar / insulin
-
very low visceral fat
-
protein sweetspot
-
circadian rhythm alignment
-
adequate NO (nitrite foods) and arterial CO2 (nasal breathing)
-
8 Likes
Bicep
#11
Looks like $3.00/day. Made from a rare seaweed. Thanks!
1 Like
Bicep
#12
Malcolm Kendrick in his book, spends a lot of time talking about the glycocalix. He says it’s made of the same stuff as glucosamine and chondroitin and they are shown to help heart disease, though nobody knows why. He thinks they supply what you need to rebuild. I’ve been taking them for a couple years, they’re cheap. I’m sure they don’t work as well.
1 Like
I would like to see an intervention study showing that.
$75 for 1 month supply
You could definitely construct it yourself.
Ingredients
1 Like
Bicep
#15
He cited 3 or 4 more about how having more albumin really helps. For every 10g/L drop in albumin, the risk of CVD doubles. Albumin is physiologically bound to the glycocalix.
"habitual use of glucosamine was associated with a 15% lower risk of total CVD events and a 9-22% lower risk of individual CVD events (CVD death, coronary heart disease, and stroke)
3 Likes
The first study is a mechanistic one showing that treating special models of mice with large quantities of chondroitin can reduce inflammation.
The second study is an observational one with usual cofounders (people who take supplements are more likely to be health conscious etc.).
I think we need an intervention trial for chondroitin showing that it can actually exert an anti-inflammatory effect similar to colchicine that leads to a direct reduction in events.
Imo chondroitin could be interesting but glucosamine appears to be worthless from existing clinical research in humans.
1 Like
The main reason I take glucosamine chondroitin is because if I don’t, my knees hurt. That’s good enough for me.
3 Likes
mccoy
#18
I have it in my listening list.That appears a good example of what I’d call 3rd order intervention.
1st order: decreaseDL/ApoB . By now it’s clear that cumulative exposure is positively correlated to events
2nd order: Check and eventually take care of: smoking, diabetes/hi BG, Elevated systolic BP. These factors, as explained in the posted article, multiply the risk of events substantially, pushing the dose-response curve dangerously upward.
3rd order: supplements and drugs as suggested by Dr Twyman, sometimes they overlap with 1st order. Arterosil HP supplements may push the dose-response curve downwards probably, I don’t know about specific studies though. They are all herbal extracts, which are beneficial anyway.
About inflammation, I wonder what are the more relevant biomarkers for atherosclerosis risk, CRP…, others? We should obviously check these as well and intervene to push down the dose-response curve…
3 Likes
Why not take Bempedoic Acid, Ezetemibe and a statin? They will lower ApoB, LDL and hsCRP. My father’s LDL went from 130 to 34 while his HDL is 61. It seems like a no-brainer for preventing CVD.
I don’t see the point in spending a lot of time trying a lot of marginal treatments that may not do much to lower LDL and ApoB to the appropriate levels when an optimal solution is right there in front of you.
2 Likes
mccoy
#20
I’m about to start a statin/ezetimibe combo soon, in minidoses. Bempedoic acid is pretty costly, the GP will never prescribe it for preventional purposes. Unless we try and use alternative suppliers, probably it’s that what you are doing?