I buy a Bempedoic Acid and Ezetemibe combination pill called Brillo EZ for 50 cents a pill from my Indian supplier, Jagdish. It took my LDL from 120 to 68. Add in 5 mg Lipitor and my ApoB and LDL became 48. It also had a similar effect for my father.
For about 60 cents a day, I can take arteriosclerosis, heart attacks and strokes pretty much off the table.
Also, having clear arteries probably has a lot of other benefits as well.
@mccoy I don’t see a reason not to go after all biomarkers outside of normal ranges. That said, I believe inflammation is the fundamental problem to solve. The post you referenced included a list of interventions I use to target inflammation. But I also take bempadoic acid.
“For myself I act as though everything that lowers inflammation is good for glycocalix:
- exercise (not too much too soon, sufficient recovery, etc)
- gut health
- low AGEs
- healthy blood sugar / insulin
- very low visceral fat
- protein sweetspot
- circadian rhythm alignment
- adequate NO (nitrite foods) and arterial CO2 (nasal breathing)”
1 Like
约瑟夫
#23
Which title?
He has authored several books.
约瑟夫
#24
FWIW
This test has been posted before;
Endothelial Dysfunction (arterial health) test.
mccoy
#25
I didn’t know that test, it may be pretty useful, but I must play devil’s advocate. The blurb they posted on their site, appears to be misleading. The main cause of atherosclerosis as discussed widely in this forum, according to medical consensus, is ApoB particles (and its proxy LDL).
That website affirms it is endothelial disfunction per se. How can we reconcile these two aspects?
Atherosclerosis, the build-up of plaques within the walls of the arteries, is caused when the endothelial cells that line the thousands of miles of blood vessels become dysfunctional. We also know that endothelial dysfunction is caused by the same heart risks that initially damage the endothelium.
Based on new clinical findings, many leading cardiac researchers now believe that endothelial dysfunction, considered as “the ultimate risk of the Cardiovascular risk factors”, is a disease unto itself and that this disease is what causes damage to the vessels of the heart, not atherosclerosis. Furthermore, this dysfunction is triggered by an inflammatory response to the damaged endothelium. Atherosclerosis, and the subsequent plaques and arterial blockages and heart attacks that it causes, are manifestations of this endothelial dysfunction.
1 Like
mccoy
#26
All right, but how do you know that you have a condition of elevated inflammation? Which markers did you measure and which are the right ones to consider? Should we prioritize inflammation if there is no evidence of it?
This aspect of inflammation is not discussed at all, or just hinted at, by Dayspring et al.
1 Like
Here is some useful information on inflammation from this paper: Inflammageing: chronic inflammation in ageing, cardiovascular disease, and frailty
Key points
-
High levels of pro-inflammatory markers in the blood and other tissues are often detected in older individuals and predict the risk of cardiovascular diseases, frailty, multimorbidity, and decline of physical and cognitive function.
-
In individuals with obesity, visceral fat produces pro-inflammatory and chemotactic compounds and is infiltrated by macrophages, lymphocytes, and senescent cells with a senescence-associated secretory phenotype that contributes to inflammageing.
-
Mechanisms potentially underlying inflammageing include genomic instability, cell senescence, mitochondria dysfunction, microbiota composition changes, NLRP3 inflammasome activation, primary dysregulation of immune cells, and chronic infections.
-
Clinical trials suggest that modulating inflammation prevents cardiovascular diseases, but studies to explore the effects on other chronic diseases, frailty, and disability are scarce and controversial.
-
Inflammageing can complicate the clinical features of cardiovascular disease in older individuals by causing an energetic imbalance towards catabolism and interfering with homeostatic signalling, leading to frailty.
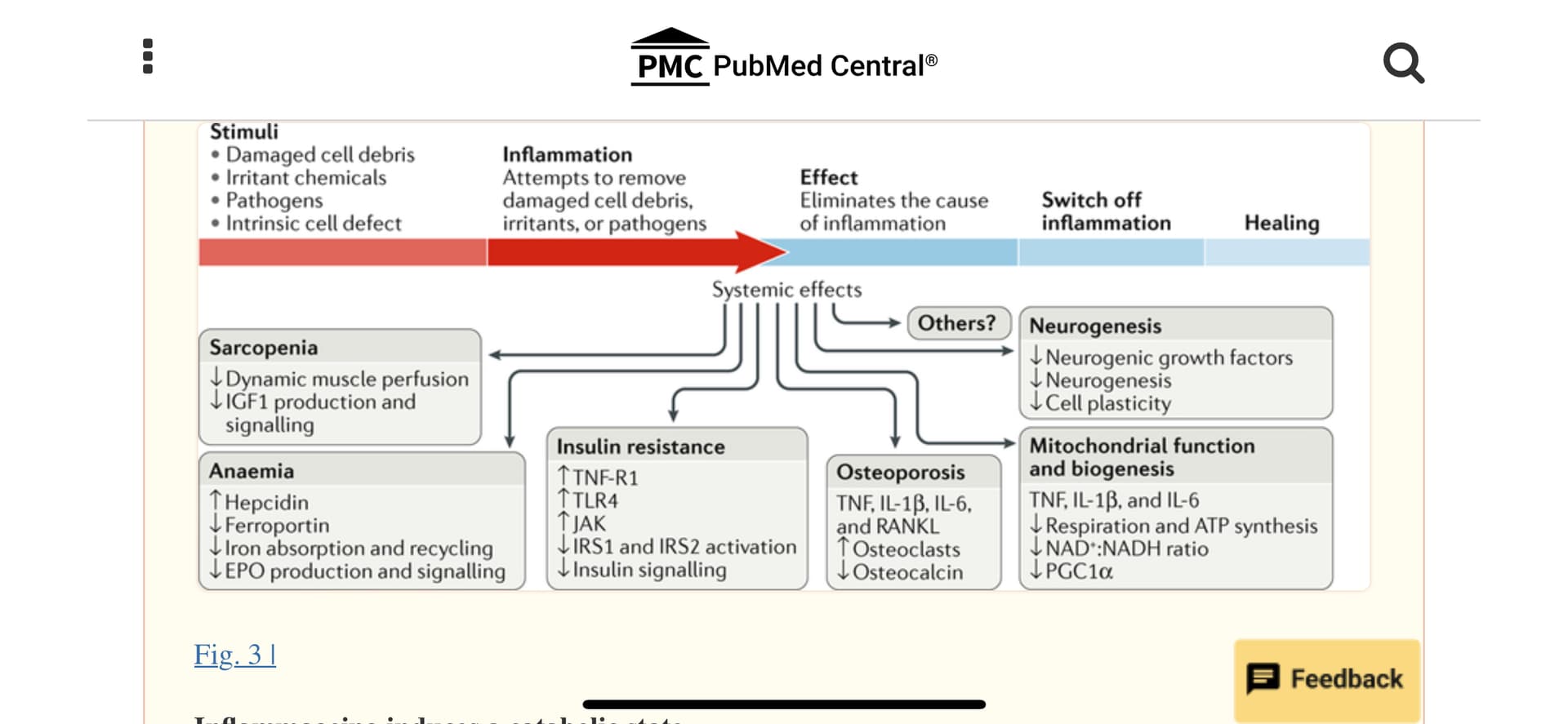
Inflammageing induces a catabolic state.
“Inflammation causes pathological states linked with frailty, cardiovascular disease, and ageing. Sarcopenia: the induction of anabolic resistance in muscle inhibits the perfusion adjustment to anabolic stimuli as well as insulin-like growth factor (IGF1) production and signalling235–240. Anaemia: chronic elevation of IL-6 levels causes anaemia through the production of hepcidin, reduction of the transmembrane iron transporter ferroportin, and inhibition of iron absorption and recycling as well as interference with erythropoietin (EPO) production and signalling3,280. Insulin resistance: tumour necrosis factor receptor superfamily member 1A (TNF-R1) and Toll-like receptor 4 (TLR4) block insulin signalling through Janus kinase (JAK) activation, which causes serine phosphorylation of insulin receptor substrate 1 (IRS1) and IRS2, contributing to insulin resistance283. Osteoporosis: TNF, IL-1β, IL-6, and TNF ligand superfamily member 11 (RANKL) contribute to osteoporosis by stimulating osteoclast growth and activity and inhibiting the production of osteocalcin290,291. Mitochondria biogenesis: studies in vitro show that TNF, IL-1β, and IL-6 induce mitochondrial dysfunction with reduced ATP synthesis-driven respiration, a reduced NAD+:NADH ratio, and reduced mRNA levels of PPARGC1A (encoding peroxisome proliferator-activated receptor-γ co-activator 1α; PGC1α), suggesting impairment in mitochondrial biogenesis287. Neurogenesis: pro-inflammatory cytokines interfere with the biological activity of neuronal growth factors, such as brain-derived neurotrophic factor, thereby affecting neurogenesis and plasticity292. Accordingly, the addition of IFNα to human hippocampal progenitor cells reduces neurogenesis289. These are just few examples of how chronic inflammation promotes a catabolic state, suggesting a possible unifying hypothesis. During an acute bout of inflammation, induced for example by an infection, the surveillance of damage and continuous repair functions in multiple tissues are chronically inhibited, leading to accumulated damage in organelles and macromolecules. Over time, this damage accumulation across different tissues and organs could become so severe that it cannot be compensated for and causes irreversible frailty.”
1 Like
Bicep
#28
Quick googling finds that insulin resistance causes endothelial dysfunction:
https://www.sciencedirect.com/science/article/abs/pii/S0002914903006118
So NO is very important, Insulin sensitivity is important, inflammation is important. I took pioglitazone for a few months, then quit because it didn’t seem to do anything.Pioglitazone is a thiazolidinedione and that’s what they’re talking about in the Science Direct article.
Using your own brain can get you into trouble. You’re just supposed to take your statin. Lol.
I’ll add that my hsCRP (roughly a measurement of Il-6, I understand) has been around 0.2 for a long time. Very low. Yet, as I have written here, after my 5-day FMD, all of my post resistance training joint soreness has vanished. I have now lifted 5 times since I first reported that effect, and it keeps going. No pain. I have even started doing sprint intervals after my workouts. No joint pain.
I assume some level of reset occurred in my immune system despite >1 year of rapa (during my diet, pet dander, and seasonal allergies disappeared) and a very low hsCRP.
I’ll bet I’m getting benefits beyond missing joint pain.
3 Likes
I bet you if statins were never patented you would be ordering them from shady nootropics pages today.
1 Like
I cannot explain this fact. My guess is two-fold:
(1) simple message for simple people (patients)
(2) inflammation is complex and hard to solve without a lifestyle commitment and almost no one will do it, so see option #1
I think statins are amazingly good at lowering apoB (I believe statins also lower inflammation). Rosuvastatin worked for me. But it did other things as well that made me feel old. I see no reason to take a statin when I have access to other tools that accomplish the same thing without ruining my life.
2 Likes
Hyperbole much. Not taking a statin can ruin your life… or rather end it for good.
@Virilius Are you claiming to know that the statin was not ruining my life? How did you come by this information?
1 Like
Because “ruining your life” is something that really screws you up for good, not a side effect of a drug that goes away within days of cessation.
1 Like
Bicep
#36
I do tend to try things. I tried a couple statins including rosuvastatin. I injected the expensive stuff that increases the number of LDL recyclers for a month or so (free trial from my doc). Can’t think of the name. I have a bunch of bempedoic acid here but haven’t started it yet. I’ve used metformin a few times. SGLT2’s are not a terrible solution, but I don’t like getting up to pee. I like the cyclodextrins.
Usually it’s best to use things as they were designed to be used. In this case that means as our ancestors lived. Active life in the sun and eating unprocessed food. Unfortunately I abused my poor system for awhile and now the question is whether any of these solutions is better than nothing. There are brilliant people on both sides. Eades teaches me something important every week. I may post on that later, this weeks was really good.
1 Like
@Virilius Sorry to offend your sensibilities on proper word usage. Yes, it only stopped ruining my life because I stopped taking the statin. If I didn’t stop it would have continued ruining my life. And I was lucky to figure it out. I had to guess that stopping the statin would have that effect, which otherwise was a mystery to me. I was never warned by my doctor or ever read anywhere that a statin could do that.
3 Likes
mccoy
#39
Guys, with all due respect but I have 2 main issues with the worries about inflammeaging, maybe I’m being dense, but .
1- This is a relatively recent model, with no guidelines, not a volume of trials even remotely comparable to the model of atherosclerotic disease caused by lipoporoteins.
2- If we are concerned about an ostensible state of systemic inflammation, we have the tools to measure it. If our markers like CRP are good, then why to worry?
My bottom line, the preponderance of evidence is that ApoB lipopoproteins circulating in blood are the main driver of atherosclerosis. Presently, all other drivers are secondary. The posted article suggests smoke, elevated SBP, diabetes as exacerbating factors. Inflammation is only cited in this article: Libby, P. Inflammation in atherosclerosis. Nature 420, 868–874 (2002).
4 Likes
Usually it’s best to use things as they were designed to be used. In this case that means as our ancestors lived.
And they all died way before they reached the age of 100. As nature intended.
Unfortunately I abused my poor system for awhile and now the question is whether any of these solutions is better than nothing.
The worse your health the more treatments you need.
@约瑟夫_拉维尔
Sorry to offend your sensibilities on proper word usage.
It does sound silly.
1 Like
A_User
#41
Yeah, as Thomas Dayspring said recently, find a statin trial that has CRP as the endpoint. Drugs are approved nowadays only if they reduce LDL, it’s that good, pending outcome trials. At the same time inflammation plays a role albeit a relatively much smaller one, so it’s still important. But biomarkers need to be weighted appropriately and LDL is so extremely good for ASCAD based on the best evidence available. No one should ignore insulin sensitivity or resistance, or inflammation, but atherogenic lipoproteins carrying cholesterol in serum is so important to prevent ASCAD.
3 Likes
Jonas
#42
Here is a trial in 2001: Effect of statin therapy on C-reactive protein levels: the pravastatin inflammation/CRP evaluation (PRINCE): a randomized trial and cohort study. Peter Attia favors Pravastatin at one point.
-
Pravastatin significantly reduced CRP levels by 16.9% at 24 weeks and 14.7% at 12 weeks in the primary prevention trial.
-
This reduction was consistent across various subgroups and was not strongly linked to changes in LDL-C levels.
-
In the secondary prevention group, similar CRP reductions were seen at both 12 and 24 weeks.
-
Key Predictors of CRP reduction were pravastatin use and initial CRP levels.
-
Conclusion: Pravastatin has anti-inflammatory effects independent of its cholesterol-lowering properties.
https://elicit.com/notebook/f117d7b8-453f-445d-ba52-5906b622624b#17f123b7e928172f923db071f7fce227
2 Likes