It would be better with atorvastatin 10 mg, as compared to rosuvastatin 5 mg in RCT it has lower diabetes risk and cataract surgery:
The rosuvastatin group had a higher incidence of new onset diabetes mellitus requiring initiation of antidiabetics (7.2% v 5.3%; hazard ratio 1.39, 95% confidence interval 1.03 to 1.87; P=0.03) and cataract surgery (2.5% v 1.5%; 1.66, 1.07 to 2.58; P=0.02). Other safety endpoints did not differ between the two groups.
Rosuvastatin versus atorvastatin treatment in adults with coronary artery disease: secondary analysis of the randomised LODESTAR trial 2023
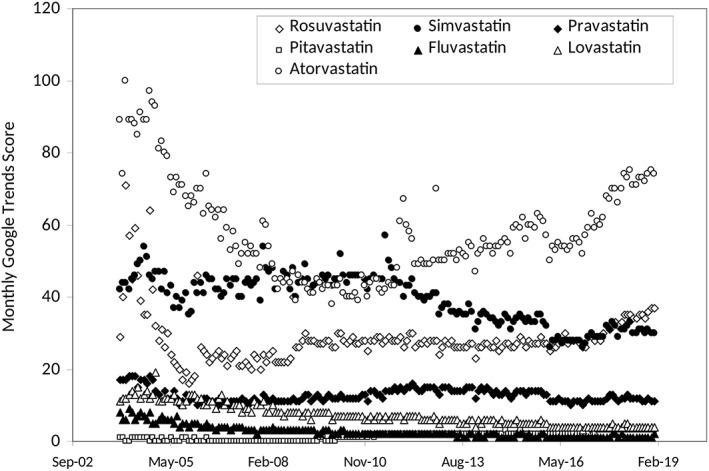
Atorvastatin is also a very popular drug on google trends, and it increased in popularity at the same time it became generic:
Statins popularity: A global picture 2019
I am quite certain there is no difference between statins based on lipophilic vs. hydrophilic status, they all cross the BBB according to Thomas Dayspring and it was really a marketing term and there is probably no clinically relevant difference in hepatoselectivity etc, with same side effects, only useful in as far different metabolism for drug-drug interactions maybe or RCT evidence. I did say earlier there was a difference, but it was regarding more vs. less hepatoselectivity. I have seen a recent study showing all statins cross the brain barrier confirming what he said, but I can’t find it. I think it was a review on statins and dementia or alzh.
Based on secondary outcomes in RCT’s, statins have either a neutral or positive effect on dementia including vascular dementia and no difference between hydrophilic/lipophilic statins according to Peter Attia based on clinical trials he reviewed in a recent premium article on statins I think.
There is speculation based on association studies long ago on serum desmosterol being associated with AD and mild cognitive impairment. Serum desmosterol is highly correlated with spinal fluid desmosterol. It is a marker of synthesis of cholesterol.
All statins cross the BBB and decrease synthesis of cholesterol. However, most cholesterol is already made in childhood and there is little synthesis in adulthood. Serum LDL etc does not enter the brain: https://twitter.com/Drlipid/status/1755985081900900367
So if anything if I can speculate since we are speculating based on association studies, those who genetically have a tendency to overproduce cholesterol (LDL, apoB?) might’ve already made a lot of brain cholesterol during the stages of life where a lot is produced, with the long half-life of 5 years. Suppressing synthesis a bit might have less of an effect if so.
I don’t either know how it affects all cause dementia in apoE4 carriers, and not many studies stratify on apoE4 status. Either way what we know with most likelihood is that statins have a neutral or positive effect on all dementia based on secondary outcomes. And then you can ride the speculation train either direction. One option is to not take statins and focus on drugs that do not apparently cross the BBB like PCSK9i, and those that don’t for sure like ezetimibe, bempedoic acid. PCSK9i, Bempedoic acid and Ezetimibe, would be most warranted if serum desmosterol decreases as it’s based on this hypothesis.
At the moment I would probably say that PCSK9 inhibitors, Bempedoic Acid and Ezetimibe is better. But that statins are pretty good as well. They all lower apoB which is most important. If money doesn’t make a difference, I don’t know if statins would be preferred to be used. It could be argued for, based on apoE4 status / family history of dementia, serum desmosterol levels, because of the amount of data that exists for them and maybe they make a different in the brain if someone is overproducing cholesterol there (vascular dementia?) (depression?) (inflammation?).
Edit: But it could be worthwhile anyway to use rosuvastatin… different metabolism allows for use with grapefruit juice, it is more potent, maybe the hydrophilic nature of it make some difference.