scta123
#202
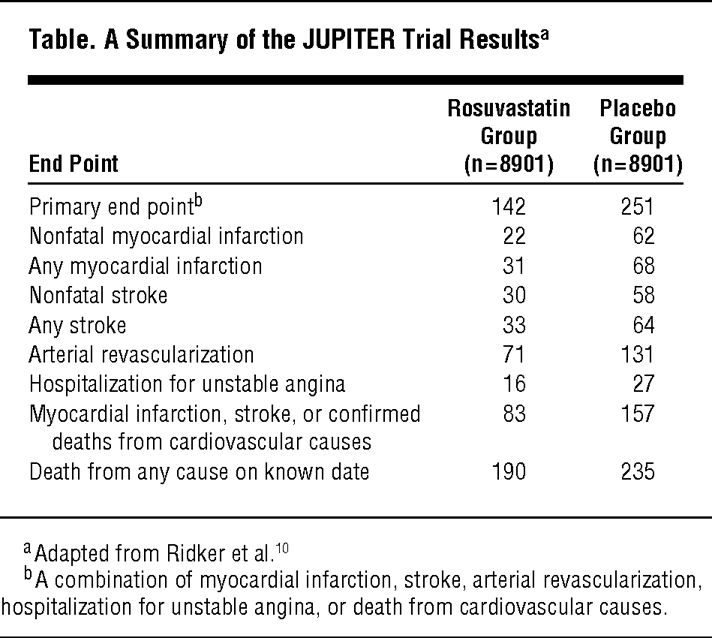
Thx. for the video. Did you find the video endorsement for statins in primary prevention? I find it the opposite. It just confirms that statins for primary prevention in low risk (Jupiter was probably all median risk) individuals does not make any sense. There was a great reference in the video as well:
2 Likes
A_User
#203
No it’s not an endorsement, it is a counterpoint like I said.
I don’t care about the JUPITER trial that much either way nor did I use it for my decision making. In fact I have not heard about it at all until recently.
It would only confirm as such if it’d be able to refute the mendelian randomization data which it cannot because of the duration of the study. And I don’t see a reason for why it would, hence it still makes sense to me.
scta123
#204
Good for you. I would still think twice. I don’t dispute that LDL-C is genetically linked with lifespan just that lowering it with drugs is more reasonable in genetic subtypes that promote higher LDL-C and especially in individuals who have additional risk factors.
At this moment I haven’t seen a convincing evidence that would support any of the lipid lowering medicine intervention that would allow saying with certainty that benefits outweighs any possible risk in low risk population. For a low risk individual trying to lower apoB burden only two medicines come to my mind as a possible interventions; Ezetimibe and fibrates. First as it does not influence cholesterol synthesis only reabsorption and the second cause they can favorably change lipid profile. Both mechanisms are safe enough IMO. Both are thus not strong in high risk population and almost useless for secondary prevention.
But saying the above, if you are medium/high risk and have unfavorable genetic burden and/or additional risk factors you should do anything to lower your LDL-C to extend your health and lifespan.
3 Likes
A_User
#205
I don’t understand what you’re saying, feels like you’re talking in riddles, be clear what you mean.
How much would that lower apoB for someone around 70-80 mg/dl?
tj_long
#206
1 Like
scta123
#207
High LDL-C = lower lifespan
Medicine intervention makes sense if your genetic subtype favors LDL-C and if you have other risk factors (metabolic disorders, high BP, diabetes etc.)
Combination? I assume 15-25% (if your are cholesterol over absorber possibly little more).
Fibrates seem interesting as they don’t move that much lipids, but particle composition. Which might be IMO better for prevention. They lower TG and favor apoA-1 particles for lipid transport. Thus reducing apoB burden.
A_User
#208
I don’t think about risk, so I guess we’re different in that regard.
scta123
#209
Yes, most damage is done from your teens to middle age. If you start in middle age with advanced ASCVD the interventions must be very radical in order to prevent future events. Maybe @A_User and others who are in their twenties must be far more hands on about it.
scta123
#210
Yes, I see you are trying to isolate LDL-C as an independent causal factor and I am trying to understand ASCVD as a far more complex degenerative disease.
3 Likes
A_User
#211
No, I think about stopping atheroschlerosis from developing in the first place. Not any risk. Not risk calculators.
scta123
#212
But it doesn’t help you much if you choose an intervention that would reduce your lifespan by some other mechanism, does it?
2 Likes
A_User
#213
Statins don’t. You can monitor diabetes risk. There isn’t any other side effect as far as I know which would qualify.
I don’t dispute that there is a role of cholesterol, but I think improper differentiation is one of the causes of ASCVD.
There is some evidence for this in the literature:
tj_long
#215
One problem is that it’s difficult to know for sure whether an individual definitely belongs to a low-risk group. Statistically there are adequate methods for this, but they do not guarantee a risk assessment at the individual level. The individual is not reassured if the criteria work at the population level but not for that specific individual.
I personally know individuals who belonged statistically to a low-risk group but developed coronary artery disease at the age of 65-70. This is also an interesting example (of course the healthiness of elite sports can be debated): https://youtu.be/9PEL9lCDjnI?si=5ecTLOqGmvMYoEVU
scta123
#216
What do you mean here?
And yes, sport, especially professional sport or elite sport is no protection for ASCVD on it’s own. Maybe even the opposite, since they appear to have more atherosclerotic plaques, but are usually more stable.
1 Like
tj_long
#217
No cardiovascular diseases in the close family, normal blood pressure, normal lipids etc. Standard risk factors for cardiovascular diseases.
1 Like
scta123
#218
Clinically assessed or self assed?
tj_long
#219
The doctor did not prescribe statins before the CAD.
scta123
#220
You know unfortunately medicine and most doctors still does not understand what is prevention and they rely on old doctrine of treating when you are already presenting symptoms. Doctors are also not gods that would know everything, they rely on guidelines and practices and rarely venture into unknown. There are of course exceptions.
Taking care of yourself and your own health and taking preventative measures takes also some investment on your own side. Investment of willingness, time and money. It is also a demonstration of self love but it is not always pleasurable.
With doctors you need to ask questions and you need to be able to hear unpleasant answers. This is sometimes the most difficult part.
Especially with ASCVD which is very complex disease preventative measures are complex too. I know that national guidelines are slow to change and full of compromises and Pharma lobbing, but now you can have this tremendous access to information and most of ASCVD is preventable, but you need to do most of the work on your own. I don’t think statins (or other medical interventions) would solve it on its own as prevention.
2 Likes
tj_long
#221
IMHO statins are just one tool, diet, sleep and exercise are more important.
5 Likes