adssx
#15
I’m not sure to understand your point.
This thread confirms that estimates (such as on the Apple Watch) can be widely inaccurate (+/- 10 mL/kg/min): https://twitter.com/nntaleb/status/1710988673771012145
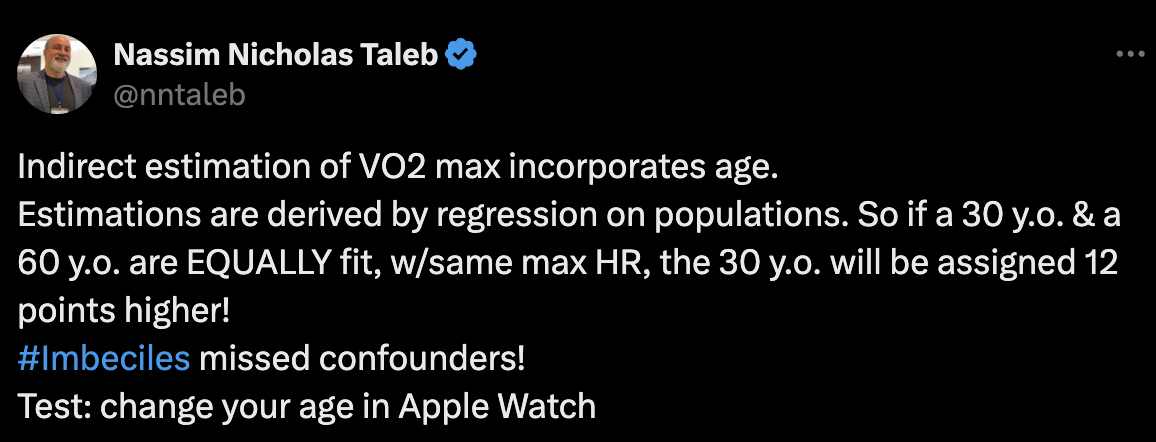
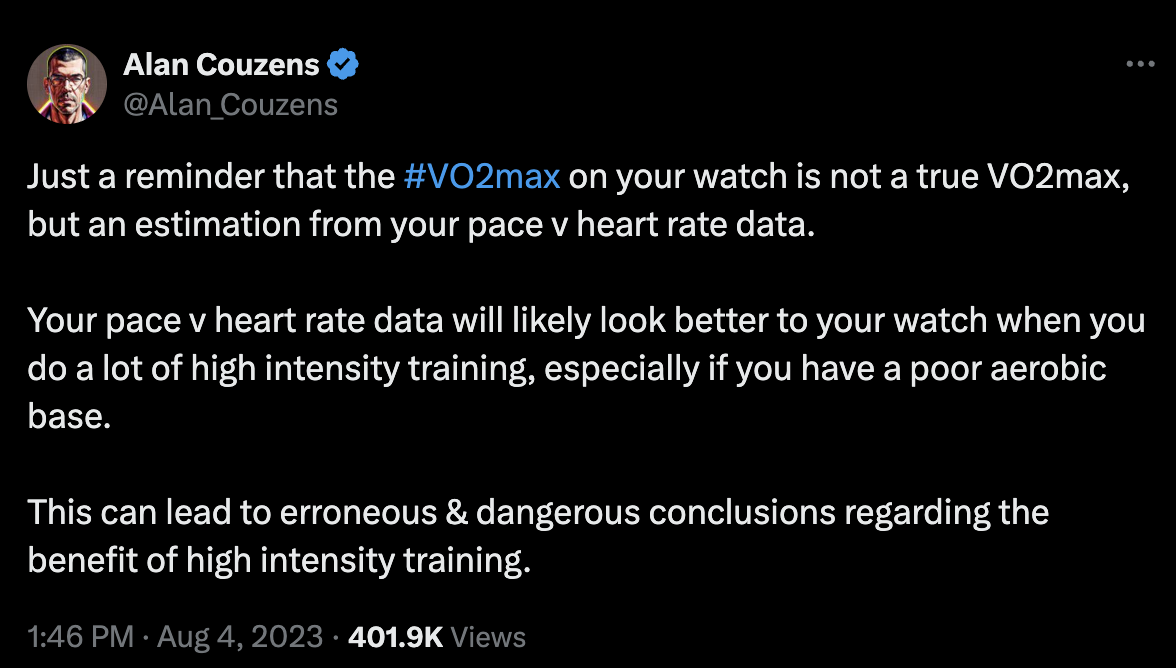
Using poor estimates can lead to mistakes: https://twitter.com/Alan_Couzens/status/1687444815439613952
So, I disagree with “from wherever you got it”.
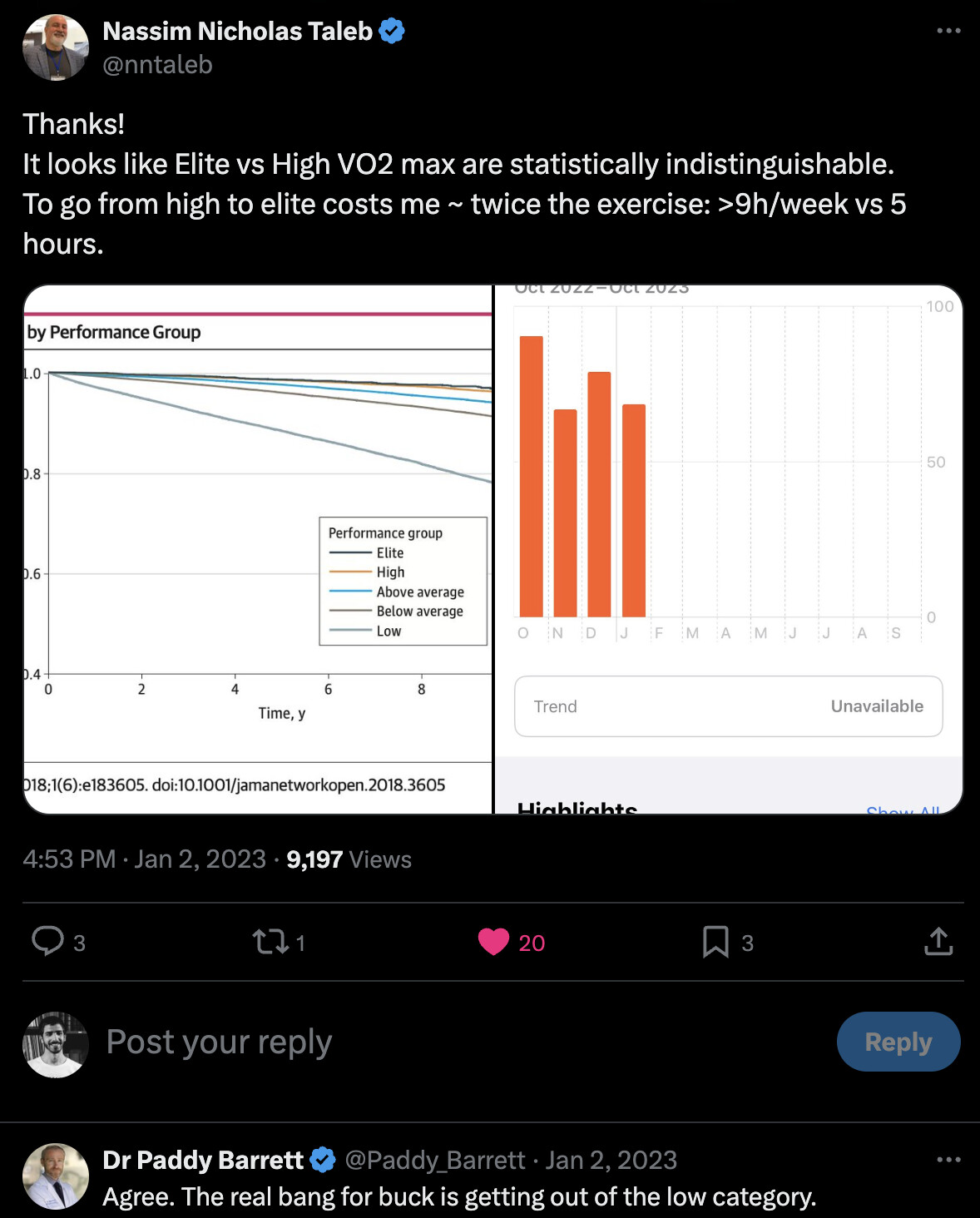
On the other hand, I agree with “What matters is that your number isn’t low”, based on this paper: Association of Cardiorespiratory Fitness With Long-term Mortality Among Adults Undergoing Exercise Treadmill Testing 2018
See Taleb’s and Barrett’s comments on the paper:
So yes, you mostly don’t want to be in the low (<25th percentile) performance group (“stratified by age- and sex-matched” in the paper).
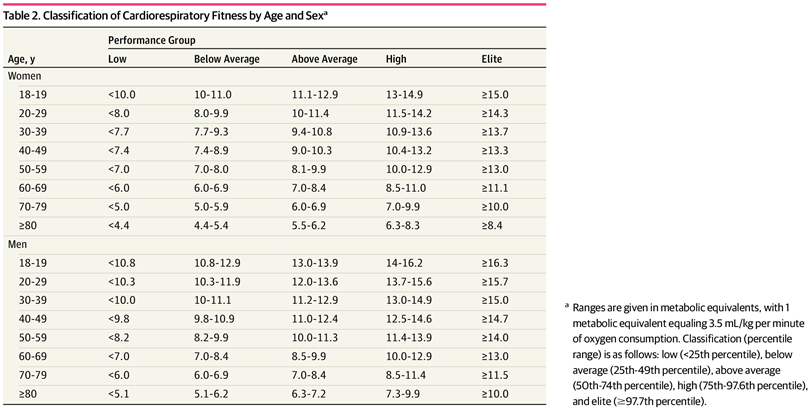
For that, I understand that you need to 1/ Measure Vo2 max in a clinic and 2/ Know the percentiles (and especially the 25% one) for your gender, age group, and exercise modality.
That paper gives the following table for peak estimated metabolic equivalents on treadmill testing (multiply by 3.5 to get Vo2max?):
Did I miss something in my reasoning?
(In any case, whatever your gender, age, and modality of exercise, Vo2 max > 38 mL/(kg·min) is always above the “low (<25th percentile)” performance group, and Vo2 max > 47 mL/(kg·min) is always above average.)
1 Like
A_User
#16
I feel like this is opening a can of worms, and there are lots of confounding factors. I’d like to see a mendelian randomization study on VO2 max specifically, with genes that aren’t in the brain, for example, to avoid pleiotropy with exercise activity. Like being in lungs or blood cells or something. I’m sure there are drugs that increase VO2 Max now or on in the future. Would such a drug be a healthspan drug?
You are accurately understanding the details involved, as far as I can tell. The question is how much accuracy is necessary. I do not think I need to go to a lab to have my vo2max measured. I can just go on a group bike ride to find out how I am doing. If I can hang (year after year) with a group of my peers, I’m doing well enough. If I had an Apple Watch and it said my vo2max was low, I wouldn’t believe it.
My thinking is I just need to have a solid level of cardio fitness and then keep it up over the years. If I am doing that, then I should invest my time and money elsewhere to my health and longevity.
1 Like
adssx
#18
Yes, based on your photo, I’m sure your Vo2 max is fine  But for those who have never exercised regularly and/or are starting their “longevity” journey, I think it’s worth measuring Vo2 max once. Anyway, I measured mine this morning in a clinic, 50.8 mg/kg/min on a bike, all good.
But for those who have never exercised regularly and/or are starting their “longevity” journey, I think it’s worth measuring Vo2 max once. Anyway, I measured mine this morning in a clinic, 50.8 mg/kg/min on a bike, all good.
2 Likes
That’s a nice value. Congrats!
1 Like
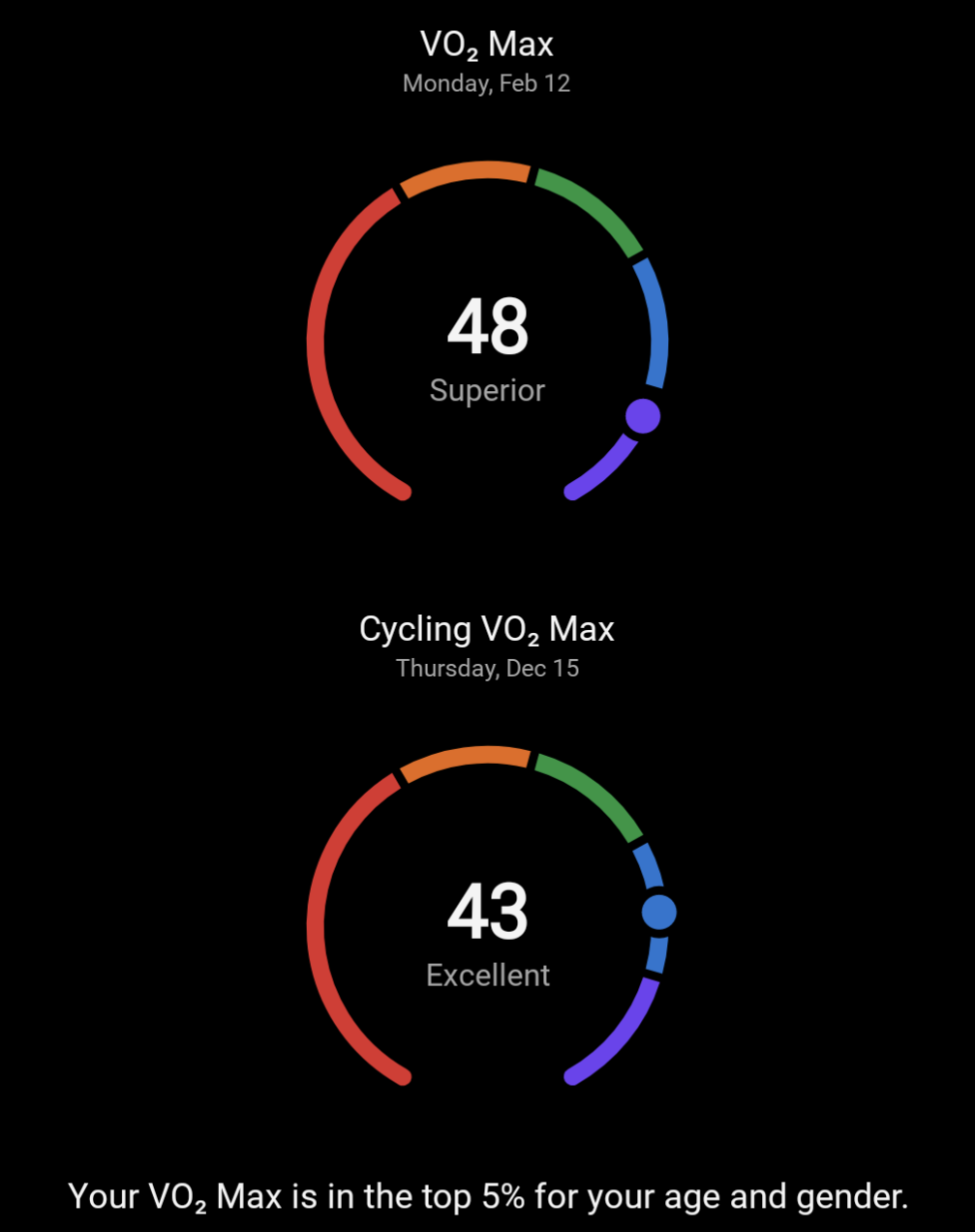
I think it’s better to know both the running/cycling VO2max values because each one tells you where you are in terms of performance in running and cycling.
For that reason you can’t have a fixed ratio for running/cycling VO2max because you could be very well trained in one or the other (or both!) sport and that would impact that ratio quite significantly.
BTW Garmin manages both running/cycling VO2max values. As you can see I’m much more of a runner than a cyclist.
2 Likes
Your referenced study (full text below)
https://digitalcommons.georgefox.edu/cgi/viewcontent.cgi?article=1021&context=hhp_fac
Data from the Ball State Adult Fitness Longitudinal Lifestyle Study (BALL ST) cohort were used for this study. The sample included test data from apparently healthy adults age 18–80 yr who performed a comprehensive health assessment and treadmill-based fitness test between April 1, 1968, and July 31, 2019
It used the Bruce Protocol developed by Cardiologist Robert Bruce. Dr. Bruce did not actually measure the VO2 max of his patients, but merely calculated it. His test was also designed to detect illness, not opitmal fitness.
Another value that can be obtained from an ETT is a patient’s myocardial oxygen uptake. This value is estimated by the product of heart rate and SBP. This rate-pressure product is important since myocardial oxygen uptake and coronary perfusion are directly correlated. Since coronary flow can increase by up to fivefold above baseline with exercise, a patient who has obstructed coronary arteries cannot meet this increased demand and ischemia results. In general, a rate-pressure product 25 000 or higher indicates that a patient has achieved an adequate workload.[10] The rate-pressure product can also be used to estimate when ischemia occurs and is a better predictor of when ischemia will develop than the exercise testing stage.[12]
Maximal oxygen uptake (VO2 max) is an additional accurate representation of a person’s cardiovascular fitness and exercise capacity, and is estimated from the peak workload achieved on an ETT. This is usually expressed in terms of a metabolic equivalent task (MET), where 1 MET is equal to 3.5 mL O2 per kg per min. The VO2 max value is affected by age, gender, baseline exercise capacity and genetics.10 Metabolic equivalent tasks (METs) can be estimated based on the protocol used for an ETT.
Dr. Kenneth Cooper actually measured the vo2 max of his study subjects. Those subjects were officers and airmen, and presumably physically fit.
To validate the 12-Minute Run Test, 115 U.S. Air Force officers and airmen were asked to run, covering as much distance as possible in 12 minutes. This was done under closely supervised conditions on a flat and accurately measured testing surface on days with mild weather conditions. Within three days after the run, all subjects underwent the maximal treadmill exercise test in Dr. Cooper’s laboratory in order to measure their maximal oxygen consumption, also known as VO2 max.
When comparing the results from distance covered during the 12 minute run and VO2 max from the treadmill exercise test, a correlation of 0.897 was found between the two. To put that in perspective, if two things are perfectly correlated (which never happens), the correlation coefficient is 1.0, so a correlation of 0.897 is very high indeed. Based on the distance covered during the 12 minute run, a very good estimate for V02 max can be made. These innovative results were published in the Journal of the American Medical Association in January, 1968.
1 Like
adssx
#22
Can you please show me which part of this paper says that estimates based on the Cooper test are equivalent to Vo2 max measured in clinic?
(of course an old paper on n=115 US Marines by Cooper himself is not reliable. Let’s be serious.)
Not your paper, but the website of Kenneth Cooper says that Dr. Cooper actually measure the airmen’s vo2 max.
Military says the same thing on their bootcamp website. Sorry. It does not allow copy and paste.
Cooper (1968) perfored this test on 115 male officers and airmen of the US Air Force, in which they were evaluated on a 12-minute field performance test, and on a treadmill maximao-oxygen-consumption test.
The correlation of the field-test data with the laboratory -determined oxygen-consumption data was 0.897; wiuth the significance oif this relationship making it possible to estimate, with considerable accuracy, the maximal oxygen consumption from only the resulst of the 12-minute performance test.
1 Like
adssx
#24
Yes, so I repeat: this is a very old study done by Cooper himself on only n=115 US male officers and airmen of the US Air Force.
It has zero value.
As of today, as far as I know, there is no large study (n>100) on people representative of the general population (males, females, different age groups, etc.) confirming that estimates based on the Cooper test are reliable. Actually, studies on this topic (and anecdotal examples) show the opposite: equations estimating Vo2 max are highly inaccurate.
If it is good enough for the airmen of the military, it is good enough for me.
The Bruce test is still employed by cardiologists. So if it is good enough for them, it is good enough for me.
I concede to not being as discriminating as yourself. A test that is not good for you, is good for the military and me.
adssx
#26
The Cooper test is great per se. It just doesn’t measure Vo2 max. And this topic is about Vo2 max. That’s it.
Also: is there evidence that, as of today, “the airmen of the military” use the Cooper test to measure Vo2 max? Or that cardiologists employ the Bruce test on a regular basis to estimate Vo2 max? (most cardiologists do not care about Vo2 max and the rare ones who do measure it in a clinic)
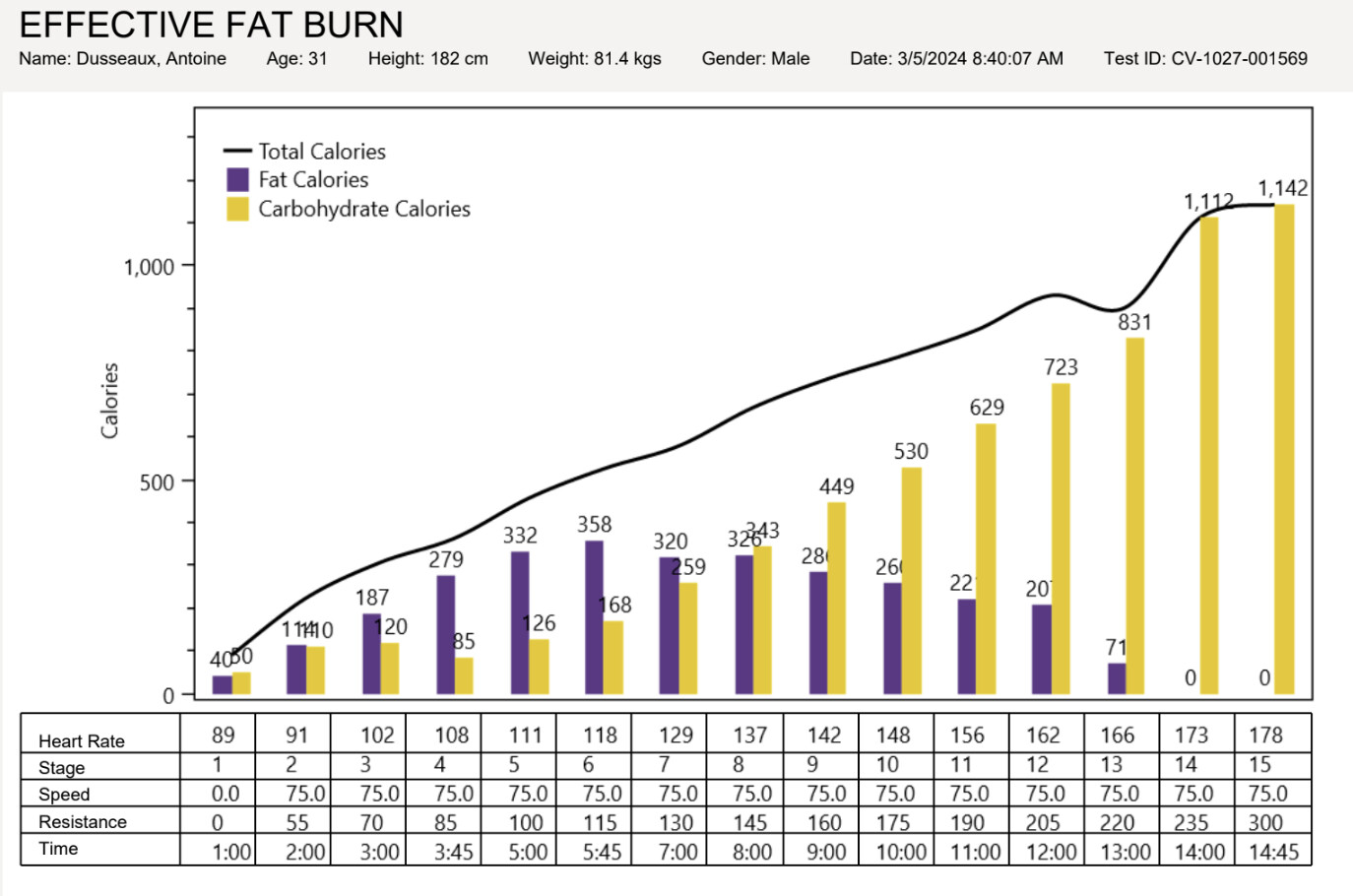
By the way, a Vo2 max test also shows whether you effectively burn fat or not:
adssx
#27
I found two papers:
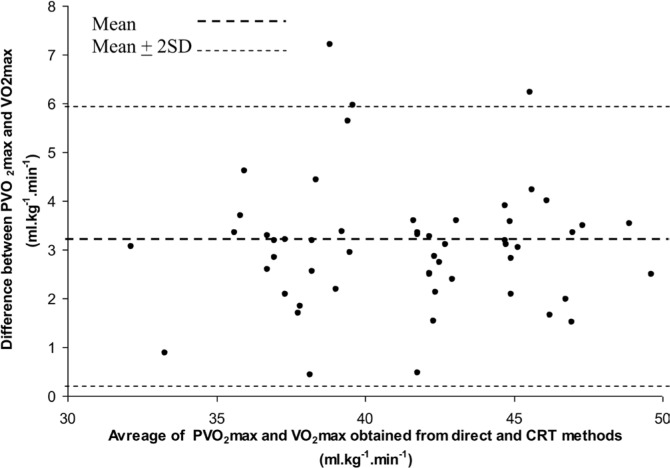
Validity of Cooper’s 12-minute run test for estimation of maximum oxygen uptake in male university students 2015 (n=88, single author from the University of Calcutta, not a great journal, but still)
(CRT = Cooper’s 12-minute run test)
Limits of agreement between PVO2max and VO2max were large enough (0.10 to 5.94 ml · kg−1 · min−1) with poor confidence intervals indicating inapplicability of the current protocol of CRT in the studied population.
Moreover, a significant (P < 0.001) difference between PVO2max and VO2max indicated that it would not be justified to accept the prediction of maximum oxygen uptake in the studied population by applying CRT as suggested by Cooper.
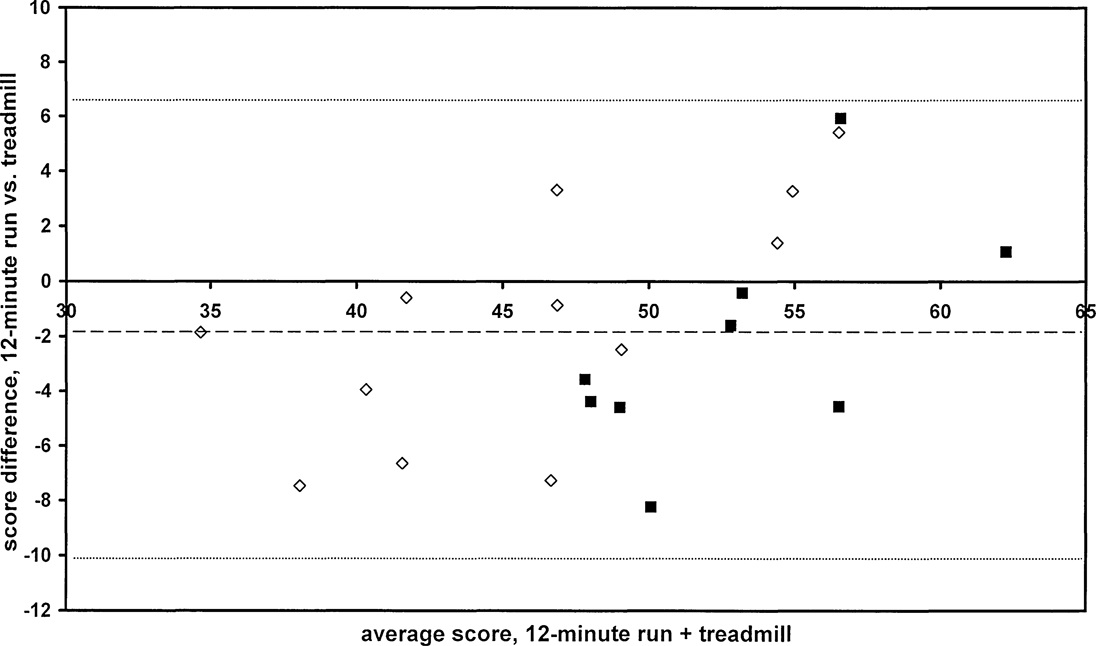
Validity and reliability analysis of Cooper’s 12-minute run and the multistage shuttle run in healthy adults 2011
However, Bland-Altman plots showed the 12MR to underestimate Vo2max scores at lower Vo2max values and overestimate Vo2max scores at higher values, a trend not observed in the MSR data.
However, the large bias at both high and low o2max values renders the 12MR of lesser use in sample populations that span a broad range of aerobic fitness levels. Currently, it appears that the 12MR can do little more than rank subjects on an ordinal scale in such a sample.
Although field test scores appear stable across test instruments and test occasions, test administrators should use caution when predicting the criterion o2max from 12MR and MSR scores. Test administrators should be particularly aware that the 12MR did not demonstrate a consistent bias across the full range of o2max values, whereas the MSR significantly underestimated TR o2max (p < 0.01).
(12MR = Cooper’s 12-minute run)
So clearly, with +/- 8 mg/kg/min difference with the clinic standard, the Cooper test is a poor estimate of Vo2 max.
1 Like
adssx
#28
It turns out that Vo2 max was discovered 100y ago, so this paper was published last week: Assessing cardiorespiratory fitness in clinical and community settings: Lessons and advancements in the 100th year anniversary of VO2max
Wearables using exercise tests show an almost negligible systematic error of 0.09 ml·kg−1·min−1, in contrast to those using resting tests, which overestimate VO2max by 2.17 ml·kg−1·min−1. Despite the higher accuracy of exercise-based algorithms, both estimation methods showed a considerable random error, with limits of agreement ±9.83 and ± 15.24 ml·kg−1·min−1 for exercise and resting tests, respectively. For clinical context, differences of <3.5 ml·kg−1·min−1 are associated with a lower risk of all-cause mortality and CVD.2,6 Even though the random error was significantly reduced in exercise-based estimates, this margin of error remains substantial. Consequently, these findings suggest that the validity of estimated CRF is acceptable at a population level (systematic error), but not yet at an individual level (random error).
Quod erat demonstrandum…
ng0rge
#29
So, you did the lab test with an O2 mask? And according to your profile, you aren’t taking rapamycin yet. I’m still not clear on the difference between taking the lab test on a stationary bike or a treadmill…since the test is measuring your cardiorespiratory system and oxygen uptake, why would the mode of exercise matter?
My reason to take the lab test is to gauge physical changes before and after taking rapamycin so I want a precise score. When you start rapamycin do you plan to take the lab test again (after a period of being on rapamycin)?
adssx
#30
Yes, my doctor does it every year to his clients.
Indeed.
I asked ChatGPT:
Yes, VO2 max values can differ depending on whether the exercise is performed on a treadmill or a cycle. VO2 max, a measure of the maximum amount of oxygen your body can utilize during intense exercise, is influenced by the muscle mass involved in the activity, the type of exercise, and the individual’s proficiency in the exercise.
When exercising on a treadmill, individuals typically engage more muscle mass compared to cycling. Running involves the whole body, particularly the large muscles in the legs, and requires significant effort from the core and upper body for stabilization and movement. This increased muscle engagement typically leads to a higher VO2 max because more muscles need more oxygen.
In contrast, cycling is more localized, focusing primarily on the legs, and doesn’t require as much upper body or core engagement compared to running. Consequently, the VO2 max values obtained while cycling are often lower than those obtained while running for the same person.
Furthermore, an individual’s familiarity and efficiency with the exercise mode can impact VO2 max values. An experienced runner might have a higher VO2 max on a treadmill, while a seasoned cyclist might achieve better values on a bike.
However, it’s important to note that these are general trends, and individual responses can vary. The best way to get accurate VO2 max readings is to test in conditions that closely resemble an individual’s specific sport or exercise context.
Makes sense to have a precise score. Treadmill vs cycle doesn’t matter for the initial test. Do you prefer running or cycling? Choose the one you’re most comfortable with and only do that in the future so that you can compare before / after.
Taking rapa is not (yet) in my plans. A few things to fix before…
ng0rge
#31
Thanks! My takeaway is to see what the lab I’m going to use does (cycle or treadmill). Then go to a gym (I usually lift weights at home) and practice a little on that. Then I’ll probably go back to the same lab to retest - or at least the same format.
The other slight wrinkle is that I live and, of course, exercise at 6,200 ft (1890 m) elevation but may have to go to sea level for the test (we don’t have it here). So my hemoglobin levels are probably higher than normal.
I thought that living and exercising at high altitude was supposed to be quite beneficial for improving VO2 Max?
ng0rge
#33
Yes, you’re right, I think the maxim for athletes is sleep high, train low (not sure why). Your blood builds up more hemoglobin in the thinner air so it can transport more oxygen through the blood system. My score should be higher at sea level. Just saying that when I retest, I need to be at the same elevation as the first test, or it won’t be a good comparison.
It’s because if you train in high altitude you have less oxygen so you are limited in the effort you can reach vs at sea level which is why you should train low.
On the other hand you need to spend a lot of time at high altitude to make more red blood cells and you make more of them at night, hence the sleep high.
1 Like