Chinese paper: Assessment of Urolithin A effects on muscle endurance, strength, inflammation, oxidative stress, and protein metabolism in male athletes with resistance training: an 8-week randomized, double-blind, placebo-controlled study 2024
We recruited twenty male individuals for this study (average age: 24.1 ± 1.59 years, average height: 177.4 ± 5.92 cm, average weight: 84.55 ± 2.72 kg, average training experience: 4.40 ± 1. 07 years), all of whom had engaged in long-term resistance training.
Participants were instructed to consume two capsules of UA(Mitopure, USA) daily(1 g/ day), each containing 250 mg of UA, after both breakfast and dinner on a daily basis.
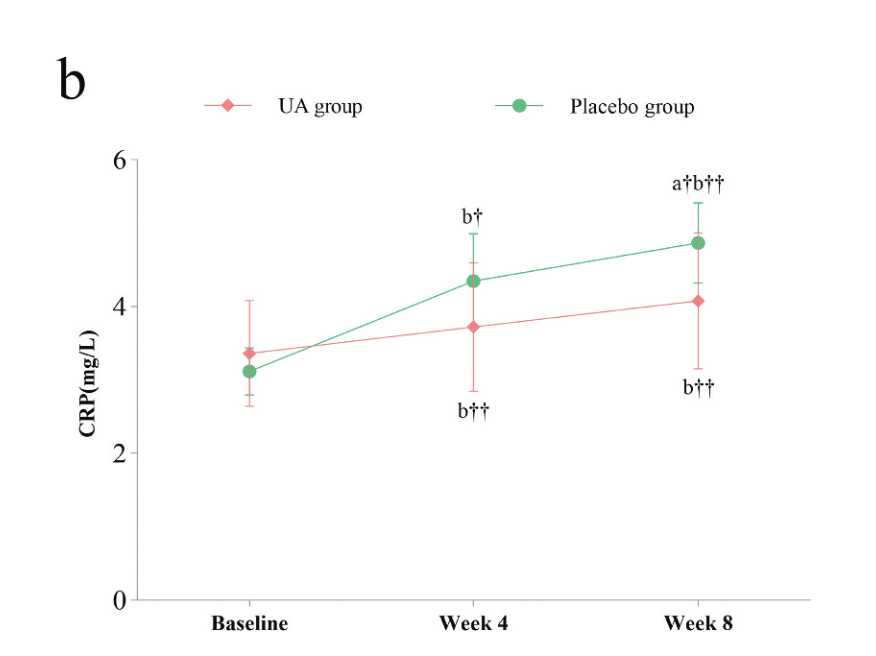
After 8 weeks of UA supplementation, compared to baseline measurements, the UA group exhibited increases in 1RM bench press and squat, although these changes were not statistically significant (Δ = 3.00 ± 0.17 kg, p = 0.051, Δ = 1.35 ± 2.73 kg, p = 0.499). However, significant improvements were noted in Maximum Voluntary Isometric Contraction (MVIC) and repetitions to failure (RTF) performance (Δ = 36.10 ± 0.62 NM, p = 0.000; Δ = 2.00 ± 0.56, p = 0.001). When compared to the placebo group, the UA supplementation for 8 weeks led to an increase in 1RM bench press and squat, although statistical significance was not reached (Δ = 3.50 ± 0.79 kg, p = 0.462; Δ = 2.55 ± 1.36 kg, p = 0.710). Furthermore, the group receiving UA supplementation, compared to the placebo group, showed significant improvements in MVIC and RTF (Δ = 43.50 ± 0.77 NM, p = 0.048; Δ = 2.00 ± 1.22, p = 0.011), indicating that the UA group exhibited superior performance enhancements in these metrics compared to the placebo group. After 8 weeks of UA supplementation, the UA group showed a significant decrease in 3-methylhistidine (3-MH) compared to baseline measurement (Δ=-2.38 ± 1.96 μmol/L, p = 0.049). Additionally, the UA group exhibited a significant increase in C-reactive protein (CRP) compared to baseline (Δ = 0.71 ± 0.21 mg/L, p = 0.001). However, there was no significant changes observed in Interleukin-6 (IL-6) (Δ=-1.00 ± 1.01 pg/mL, p = 0.076), or superoxide dismutase (SOD) (Δ=-0.004 ± 0.72 U/mL, p = 0.996) compared to baseline in the UA group. When compared to the placebo group, there was no significant difference observed in 3-MH in the UA group (Δ=-3.20 ± 0.31 μmol/L, p = 0.36). In terms of inflammation markers, the UA group exhibited a significant decrease in CRP (Δ=-0.79 ± 0.38 mg/L, p = 0.032) compared to the placebo group, whereas there was a decrease in IL-6 without statistical significance (Δ=-1.75 ± 0.45 pg/mL, p = 0.215). Furthermore, the UA group showed a significant decrease in SOD compared to the placebo group (Δ=-4.32 ± 0.90 U/mL, p = 0.041).
After 8 weeks of UA supplementation at 1 g/day, resistance-trained male athletes showed improvements in muscle strength and endurance. Additionally, UA supplementation was also associated with reduced oxidative stress levels and a decrease in inflammation response levels.
So CRP increased in both groups but more so in the placebo?