I strongly disagree. Rapamycin doesn’t fully inhibit mTOR even at high doses. It only inhibits it partially. When you’re already inhibiting mTOR with fasting, rapamycin is not likely to inhibit it much more. Rapamycin is going to have a much bigger relative effect on mTOR when you’re eating normally rather then on days you’re fasting because when mTOR is already inhibited, there isn’t going to be room for much more inhibition.
2 Likes
This is obviously false, otherwise fasting would produce the same lifespan increases that rapamycin does, but that doesn’t appear to be the case.
Almost everything in nature is cyclical; it’s only a hunch, but I’ve seen nothing to make me reconsider my suspicion that brief, but profound, suppression of mTOR is going to produce better results than a more consistent, but shallower suppression.
1 Like
I disagree. Calorie restriction does increase life span as much as rapamycin, and calorie restriction inhibits mTOR. I bet you won’t get much additional benefits from adding rapamycin to calorie restriction.
Brief but profound suppression is what you get with either fasting or rapamycin. It’s unlikely you’ll get much stronger inhibition with both together than with fasting alone. We already have studies showing that rapamycin most likely doesn’t significantly inhibit mTOR when insulin is already very low, which suggests it won’t inhibit it more when fasting because insulin will already be low when fasting.
1 Like
If CR extended life as much as rapamycin, there would be no need for rapamycin. Longevity experts would simply tell you to fast. I am a proponent of fasting, but I’ve seen no evidence that it’s going to get you to 120 years old.
And I disagree you get profound suppression of mTOR with fasting. All the papers I’ve seen indicate that it’s unlikely you see much additional autophagy with less than 72 hours of fasting. That’s when it starts. I don’t know many people who are willing to fast for 96 hours or more to maximize autophagy from fasting, so it’s unlikely many people are getting much in the way of increased autophagy.
I have also seen a couple of studies indicating that administration of rapamycin and CR ar associated with different sets of physiological effects. I very much doubt rapamycin is exerting its effects by being “fasting in a pill.”
CR is a U-shaped curve depending on your biology. One size does not fit all. There’s a fine line between optimal longevity and decreased lifespan from CR. I, for one, am not willing to try that!
Rapamycin may have negative side effects from overdosing, but it’s definitely a lot more pleasant than CR to do! Give me Rapamycin over CR any day… or just once a week. 
2 Likes
I like to cycle things. I prefer to fast at the same time as taking Rapamycin.
Although It may not double the effect in terms of encouraging autophagy, it is likely that more autophagy occurs because of a combination of Rapamycin and fasting that one in isolation.
On a cyclical basis I would wish to see a higher proportion of mitochondria recycled and replaced with more efficient mitochondria as otherwise some are likely to languish in oxidative stress for a long time.
Also I think the key for cellular health is the total response to the ATP/ADP gradient for which you need to maximise the number of efficient mitochondria in any one cell.
1 Like
There is no need for rapamycin in those that practice CR. And no they wouldn’t tell you to simply fast. They would tell you to do CR, and that’s what I and many others recommend. Only problem is almost nobody wants to practice CR (me included). Fasting is not enough. You need to actually reduce your total calorie intake a lot.
It’s not, but neither is rapamycin or CR. If you think rapamycin will get you to 120 you’re in for a disappointment.
That’s not correct. Autophagy doesn’t really start only at 72 hours. It’s not an on and off switch. It’s always on, just more gradually more when you fast. Even fasting for half a day or one day is likely to increase it a good bit. I don’t know what papers you’re reading but you don’t even need papers to figure out you you’re wrong here. Some basic physiology is enough. The depletion of liver glycogen in less than 24 hours is almost certain to indicate a gradual increase in autophagy during a 24 hour fast.
1 Like
I too think cycling is good with mTOR, even though in general it’s best for it to be reduced overall, some cycling is likely good.
I used to think the same, that is, that combining rapamycin and fasting will increase the mTOR inhibition and autophagy by a good bit (and that combining them would be great for periodic maximum mTOR inhibition), but I then I largly changed my mind when I realized two things. One is that rapamycin only partially inhibits mTOR even at massive doses, so if you’re reducing mTOR with fasting and take rapamycin the additional effect of rapamycin will be much smaller and in some cases not significant. Secondly, I haven’t seen studies that show that rapamycin inhibits mTOR further during fasting or increases autophagy further during fasting. But I have seen a human study that shows that rapamycin inhibits mTOR only when insulin is not very low. Which means, unless you have severe insulin resistance or something that leads you to have high insulin levels even when fasting, rapamycin likely won’t inhibit mTOR much at all when you’re fasting. Here is the study I’m talking about: The Mammalian target of rapamycin pathway regulates nutrient-sensitive glucose uptake in man - PubMed
Now if anyone can show me studies that shows that rapamycin inhibits mTOR or increases autophagy a good bit more when one is fasting and when insulin levels are already very low, I might change my mind. Until then, the evidence I’ve seen indicates that it will have minimal additional effects when fasting. If anyone knows of more studies on the combination of fasting and rapamycin on mTOR or autophagy, please post.
A can see a potential for taking rapamycin during fasting in people that for some reason have such poor health that they don’t manage to get sufficient mTOR inhibition from fasting. Perhaps people that have very poor insulin sensistivity so their fasting glucose and insulin are high. In such people maybe rapamycin is more likely to have additional effects when fasting.
1 Like
In the paper it you cite says: “Some limitations of our study must be considered. First, because of the long half-life of the drug and potential adverse effects, the dose of rapamycin administered to healthy volunteers was not higher than generally recommended for initiation of immunosuppressive therapy after
renal transplantation (43). It turned out that this single oral dose leads to circulating concentrations of rapamycin (9nmol/l) that were very likely not sufficient to completely
inhibit the mTOR/S6K pathway.”
Which I think would give quite a bit of leeway for fasting to cause further inhibition - at the dosing levels we tend to use.
this is an interesting point in the paper:
“Furthermore, rapamycin has deleterious effects on pancreatic islets in vitro (46).”
- Bell E, Cao X, Moibi JA, Greene SR, Young R, Trucco M, Gao Z,
Matschinsky FM, Deng S, Markman JF, Naji A, Wolf BA: Rapamycin has a
deleterious effect on MIN-6 cells and rat and human islets. Diabetes
52:2731–2739, 2003
I have not, however, found what you are saying in the paper itself.
I have seen a human study that shows that rapamycin inhibits mTOR only when insulin is not very low
I am not saying it is not there, but would as you point me at the right paragraph.
1 Like
Good point. Yes the dose administered is probably too low to cause maximal mTOR inhibition that can be achieved with rapamycin. However the dose was 6 mg, which is similar to what many are taking. It’s possible that taking 2-3 times more than that has some additional effect on mTOR when fasting, but I wouldn’t expect more than a small effect at best given that 6 mg had no effect. Expecting more than a small effect would be based more on hope than logic IMO.
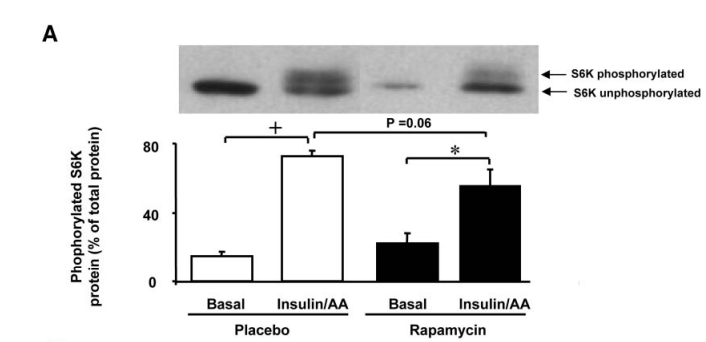
With respect to where what I’m saying is in the paper, that’s a good question. It’s not so obvious. It’s Figure 4. A in the full text. Here it is:
It shows phosphorylated S6K during fasting and fed state. It’s obviously a lot higher during the fed state and decreases modestly with rapamycin. During the fasting state, it’s already a lot lower than even the fed+rapamycin state. Rapamycin didn’t significantly influence phosphorylated S6K during the fasting state. If anything, there was a slight non-significant trend in the direction of rapamycin increasing the phosphorylation of S6K, which suggests that it had a tendency to increase mTOR1 not decrease it, in the fasting state.
Note that mTORC1 directly phorphosylates S6K so phosphorylated S6K is a very strong proxy for mTORC1 activation.
The figure also suggests that overnight fasting appears to inhibit mTOR much more strongly than 6 mg of rapamycin. That leads me to think that perhaps the benefits of rapamycin are not so much caused by it leading to periods of maximal mTOR inhibition and instead more caused by it reducing the unnecessary daily spikes in mTOR or the daily area under the curve for mTOR. One thing is for sure, we need a lot more studies measuring mTOR activation in different conditions with or without different doses of rapamycin.
3 Likes
I don’t agree with much of what you write (what is an overnight fast? That’s not nearly long enough to do anything), but I will say your last conclusion is not supported by any available evidence. The animal studies showing long lasting benefit/protection from short courses of rapamycin administration are a direct contradiction to the statement that “this leads me to think that perhaps the benefits of rapaamycin are not so much caused by it leading to periods of maximal mTOR inhibition and instead more caused by it reducing the unnecessary daily spikes in mTOR or the daily area under the curve for mTOR.”
Much of what you write also assumes that the benefits of rapamycin are mediated entirely by autophagy, and I think there’s good reason to believe this is NOT the case.
This is perhaps the key point in your post. There are quite a wide range of how biochemical systems interact with each other and that can give the perception of a chaotic system. Exactly how mTOR and S6K interact is interesting. The hyperinsulin is also hyperaminoacidemia.
If we are measuring the effects of inhibition of mTOR logically if we look at the effects of mTOR this will only be visible if mTOR was activated. In this paper that is the Insulin/AA column.
It is a bit odd that the Basal rapamycin level is higher than placebo, but that could be the rebound effect interacting with a feedback system somewhere. I have tended to think that Rapamycin might cause cells to create more mTOR complexes. (making the assumption that there is a system which manages the number of mTOR complexes functioning). This would fit with that hypothesis.
I still think that if one is in a fasted state and then take Rapamycin that the Rapamycin will add to autophagy. I tend to think of infrequent cycling of this process rather than a weekly cycle. I take the view that the key to driving mitochondrial efficiency is the maxiumum percentage of mitochondria being recycled. I am, therefore, looking at additional tools for activating AMPK at the same time as fasting and taking Rapamycin all of which would tend to increase the peak of autophagy.
I don’t think Rapamycin would reduce the peak of autophagy.
Of course it’s enough. Overnight fast is when you do something in the morning and haven’t eaten since the evening before. Usually that’s 12 hours of fasting. That’s definitely enough to influence mTOR. You don’t need long fasts to start effecting mTOR. mTOR is constantly changing throughout the day, fluctuating up and down between meals. So of course a 12 hour fast will influence it a lot. I’m not arguing that a 12 hour fast will lead to some very close to maximum inhibition of mTOR, I’m saying it definitely influences it significantly.
No, there is no contradiction there. The animals are being given rapamycin in their diet. They are getting it with food, not when fasting. The obvious implication from that is that taking it with food is beneficial. There are no studies showing that taking rapamycin specifically while fasting is beneficial for longevity.
I don’t know how you got to that conclusion. I never said that. Autophagy is one of the main benefits but not all of it.
I also think it’s more likely to do so than not. I just think the effect will be small so I consider it a bit of a waste to take it during fasting
I don’t think so either. The effects in the study above in the fasted state were not significant, so the difference might as well have been caused by small fluctuations in biochemical pathways.
“Of course it’s enough. Overnight fast is when you do something in the morning and haven’t eaten since the evening before. Usually that’s 12 hours of fasting. That’s definitely enough to influence mTOR. You don’t need long fasts to start effecting mTOR. mTOR is constantly changing throughout the day, fluctuating up and down between meals. So of course a 12 hour fast will influence it a lot. I’m not arguing that a 12 hour fast will lead to some very close to maximum inhibition of mTOR, I’m saying it definitely influences it significantly.”
Cite your source. I don’t believe you. You don’t even return to basal metabolic values for several hours after a meal. 12 hours of not eating results in a “fast” of no more than about 9 hours. That’s pathetic. You have almost as much liver glycogen when you get up in the morning as you did when you laid down. mTOR may fluctuate with your circadian rhythm, but it’s NOT due to overnight fasting.
“No, there is no contradiction there. The animals are being given rapamycin in their diet. They are getting it with food, not when fasting. The obvious implication from that is that taking it with food is beneficial. There are no studies showing that taking rapamycin specifically while fasting is beneficial for longevity.”
Straw man argument. You didn’t reply to what I wrote.
It comes down to the question as to how to maximise the proportion of mitochondria that are functioning at a higher level of efficiency.
I think to acheive that requires autophagy to be running at the highest reasonable level. I think the difficulty at a lower level is that certain mitochondria remain unrecycled whilst also inefficient.
My view on autophagy is that we need the equivalent of a Spring clean every so often. It may be worth combining a number of interventions to maximise the effect and therefore the proportion of mitochondria recycled in any one cell.
I don’t need to cite sources. This is basic biology. Besides, the study I posted above pretty much shows that mTOR is much lower after an overnight fast. Are you ignoring that study? How about you provide some evidence that contradicts that study and shows that mTOR is not lower after an overnight fast?
Almost is not the same! And it keeps gradually decreasing the longer you fast. mTOR is not an on and off switch that is on when your liver glycogen is 100%, 90%, 80% etc. fulll then suddenly turns off when your liver glycogen reaches 0% or some particular very low number. The effect is gradual. You will have lower mTOR in the morning than after eating the evening before.
Yes I did. I may have misunderstood what you’re refeferring to when talking about a contradiction. So if you want a better response, then please explain what it is exactly that you find contradicting in what I said and why.
I don’t agree to that, but I understand that you think so, given the theory you believe on the importance of mitochondria in aging.
1 Like
As a matter of interest what are your views as to the role of mitochondria in aging/protein production etc. I see mTOR as being secondary to this question of how good the cells are at producing proteins.
“Phosphorylation of mTOR was significantly decreased after 72 hours fasting”
Fasting Increases Human Skeletal Muscle Net Phenylalanine Release and This Is Associated with Decreased mTOR Signaling.
And no, you did not at all address the fact that brief treatments with rapamycin show lasting benefit. This is directly at odds with your contention that it is regular suppression of mTOR that provides the benefits from rapamycin.
Another way to ask the question is when is the best time to do a 24 hour fast? Is it during the catabolic portion of the cycle (at rapa dosing) or at the anabolic portion of the cycle (far from the rapa dose)? I would argue that I don’t want to inhibit my anabolic activity with a fast so I’ll fast around my rapa dose. I get multiple benefits from fasting aside from mTOR impacts. I also cycle my protein and my resistance training the same way. Not on/off, but higher vs lower.
2 Likes
This study is useful in showing reduction in mTOR after a 72 hour fast. However it does in no way contradict the one I posted that showed that mTOR is inhibited after an overnight fast. So I don’t see your point. Please post something that demonstrates that mTOR is not inhibited after shorter fasting, or else you have no basis for your statement and are just wasting my time.
You didn’t say exactly that it’s the long lasting benefits from short courses that you think contradicts what I said so maybe I misunderstood you. Now that I finally know that’s what you’re referring to, I can state that I disagree. Perehaps you misunderstood me. When I said the benefits of rapamycin might be caused by a reduction in daily mTOR spikes or mTOR area under the curve, that doesn’t mean I think you must inhibit it every day for years to get benefits. I never said you can’t get somewhat long lasting but smaller benefits from shorter courses of rapamycin. What I was originally trying to say is that the benefits might be caused more by reducing mTOR levels when they are high, instead of further reducing them when they are already low. I said nothing about how often this is needed for benefits.