Neo
#6
Thanks. I tried to look into it. Is this the paper?
If so please, please note that (a) the paper is just association based and (b) the authors of the paper seem to be saying that low levels can be a suggestion that there is a disease process going on.
Ie it can be a good warning sign if it starts dropping. But that is not the same as as low levels are bad in cases where such diseases processes are not going on.
Ie they seem to be saying that certain disease > low HbA1c and not just HbA1c > disease or mortality.
Think we have to be very careful when drawing causal inferences for association or correlation data.
The abstract says:
Participants with a low HbA1c (<4.0%) had the highest levels of mean red blood cell volume, ferritin, and liver enzymes and the lowest levels of mean total cholesterol and diastolic blood pressure compared with their counterparts with HbA1c levels between 4.0% and 6.4%.
So it might for instance be that people who have severe liver disease or liver cancer (together a quite large part of the population) end up with lower glucose (because the liver is the master controller of glucose).
If so it would be
Liver disease > mortality
and
Liver disease > low HbA1c
And while that means the
low HbA1c correlates with the mortality
HbA1c is not the causal driver which in this example is the liver disease
2 Likes
Neo
#7
I read a little bit more in the paper and what is was saying seem to be the perspective of the authors too?
Very low HbA1c values among persons without diabetes may reflect underlying biological processes.
Certain health conditions that decrease erythrocyte life span (eg, iron-deficiency anemia) are known to alter HbA1c values and make them unreliable
That means that such diseases are not only probably part of some of the mortality but they H1c is not even measuring their actual average glucose levels, but giving a read out that is lower than their actual glucose exposure…
Clearly that is not relevant for most of us who don’t have any artificial lowering of how long our red blood cells live?
little is known about other biological factors that result in low HbA1c values among individuals without diabetes. Low HbA1c may not reflect metabolic control among individuals without diabetes but may be reflecting other biological factors, such as red blood cell markers, inflammation, or decreased liver function
Hence it is inflammation, liver disease etc that drives low H1c and mortality
H1c hence ends up correlated with mortality but not causally
Please let me know i was looking at the wrong paper or if I am missing something
2 Likes
Your liver targets a level of about 5.0 or higher for HBA1C. If you try to lower it significantly below that, it is a sign of disease as your liver tries but cannot increase glucose release into the blood. Here’s another study that recommended 5.0.
IMHO, 4.6-4.9 is fine as well. Things start to get a bit iffy when you drop into the 4.0-4.5 range and it’s a warning sign when it drops to below 4.0.
4 Likes
Neo
#9
Thanks. I’ll take a look.
1 Like
Neo
#10
I’ll try to look into this a more after I get back from travel. But don’t think that cut off is correct. Peter Attia’s calculation is that 4.6% represents estimated average glucose levels of 85 mg/dL. That does not look like a level that is too low for the liver in a person who is optimized from a metabolic perspective and easily can utilize fat and not just glucose as energy.
From below you can also see that Peter does not seem to feel that HbA1c is 4.6% is negative.
Glucose control lives on a spectrum, but it conventionally gets lumped into three distinct categories: normal glucose tolerance, prediabetes, and diabetes. For example, whether your HbA1c is 4.6% or 5.6%, both are considered “normal” because they both fall under the diagnostic threshold of 5.7%. Once it hits 5.7%, so long as it does not exceed 6.4%, now you’ve got impaired glucose tolerance, also referred to as prediabetes. Once you’ve eclipsed the latter, whether your HbA1c is 6.5% or 12.5% (or even higher), you’re categorized as having type 2 diabetes. In most cases of type 2 diabetes, an individual traverses from one bucket to the next as their HbA1c slowly climbs from normal to impaired to outright diabetic. This doesn’t happen overnight, but too often it’s only confronted when the diabetes or prediabetes threshold is reached at a snapshot in time. Progressing from an HbA1c of 4.6% to 5.6% represents estimated average glucose levels climbing from 85 to 114 mg/dL.
This is where the CGM is more useful than HbA1c. Whar we want are spikes postprandially under 8/140. Then a drop back to 5 or slighrly less.
2 Likes
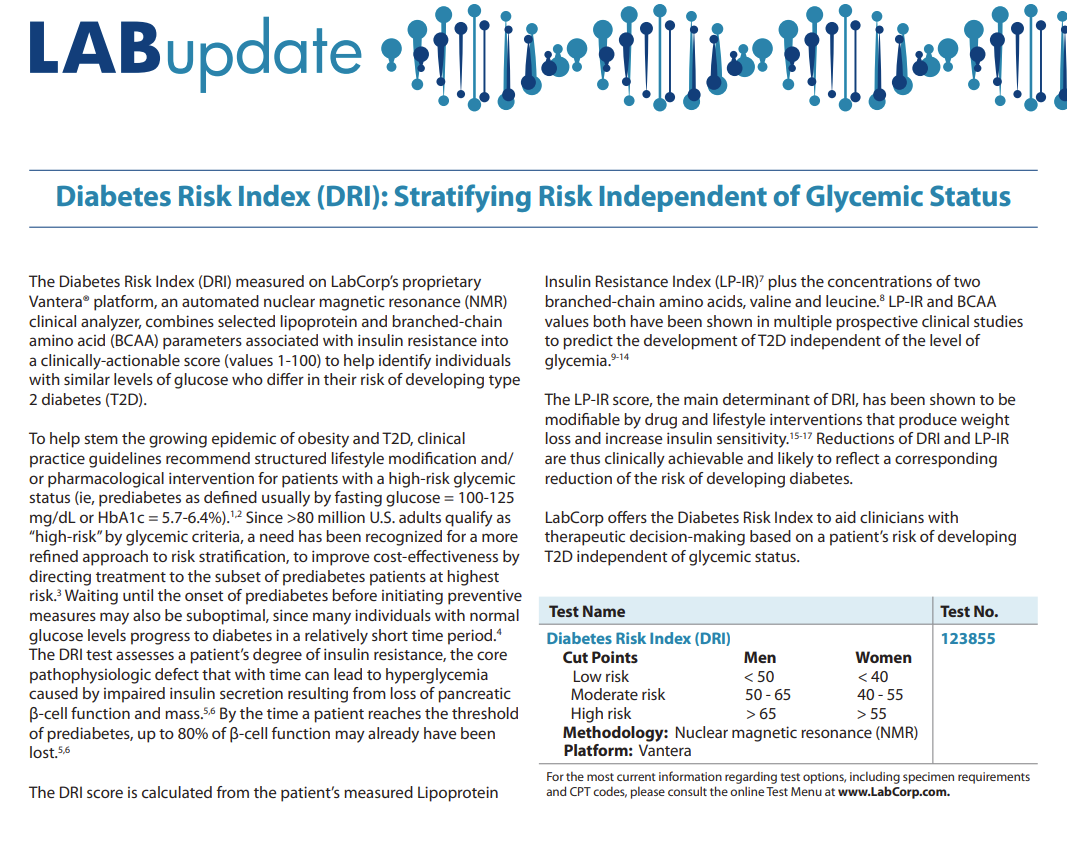
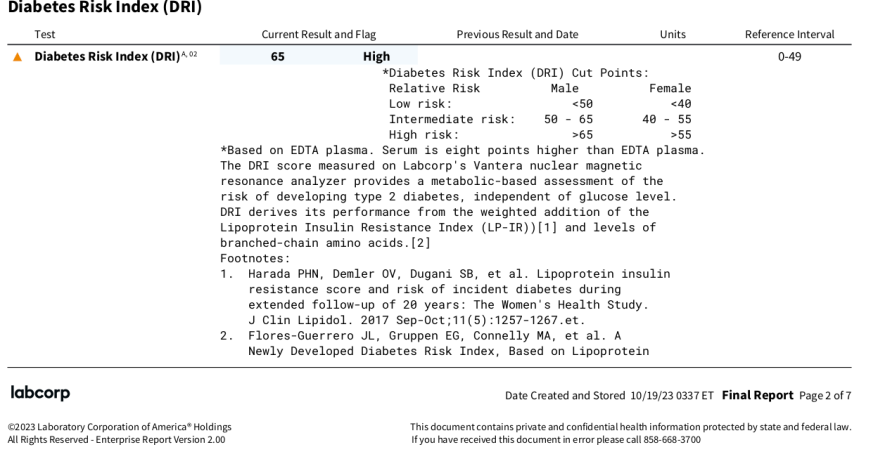
Diabetes Risk Index (DRI)
LabCorp has this test:
https://www.labcorp.com/assets/17270
My result came back with a value of 65, on the cut point between moderate and high risk. This, concurrent with an A1C of 5.4, and fasting glucose in the high 80s, which in isolation wouldn’t seem to imply much diabetes risk.
From the LabCorp writeup:
The LP-IR score, the main determinant of DRI, has been shown to be
modifiable by drug and lifestyle interventions that produce weight
loss and increase insulin sensitivity.15-17 Reductions of DRI and LP-IR
are thus clinically achievable and likely to reflect a corresponding
reduction of the risk of developing diabetes
Briefly looked at the footnoted studies, and it seems I might consider losing weight, chugging olive oil, and going vegetarian. Need to get those polyphenols up!
One might consider doing this test to confirm/disconfirm what they think they already know from A1c
1 Like
Neo
#13
And here he gives his view on that lower average glucose is better and puts that in context of success with a patient who came down to 84 mg/dL and hence at or below a predicted 4.6% HbA1c:
To recap my position and interpretation of the data available (more of which you can find in the AMA 24 show notes), lower is better than higher when it comes to average glucose, glucose variability, and glucose peaks, even in nondiabetics. In other words, there’s a lot of evidence suggesting that people with glucose in the normal range can benefit from lowering their numbers.
Let me give you an anecdote, among several I could share, to demonstrate why I find CGM useful in nondiabetics. I have*** a patient who came to me with normal glucose tolerance by standard metrics. He began CGM and after about two weeks it revealed an average glucose of 104 mg/dL over that time***. The standard deviation in his glucose readings, which is a metric of glucose variability, was 17 mg/dL. He averaged more than five events per week in which his glucose levels exceeded 140 mg/dL. All three of these metrics are considered normal by conventional standards, but does that mean there’s no room for improvement? I like to see my patients with a mean glucose below 100 mg/dL, a glucose variability below 15 mg/dL, and, as noted above, no excursions of glucose above 140 mg/dL. After about a four-week intervention that included exercise changes and nutritional modifications his average glucose fell to 84 mg/dL, his glucose variability to 13 mg/dL, and he had zero events exceeding 140 mg/dL. If he can maintain this way of living in the long-run, it’s likely to translate into an improvement in healthspan and reduce his risk of glucose impairment.
1 Like
Honestly, I think the sweet spot is 4.6-5.3. I have no idea where I fit in now that I increased my Metformin to 500 mg daily. Hopefully, I’ll be in that sweet spot. I had been thinking about adding empagliflozin, but I am concerned it may drop me into the low 4.0s which I am concerned about. Is there a bottom limit that the SGLT2is won’t drop you below?
1 Like
Neo
#15
I think they kind of hit the spikes more than the average and higher levels more than lower levels. Perhaps check the thread on Cana / SGLT2i.
Perhaps wear a CGM when you begin and then if you were to fall too low you can
- short term/intra day make sure to increase carb intake and then
- near term / between days lower the dose (eg cut a half pill, or given what people said on the other thread about the half life start doing eod dosing)
2 Likes
Kandice
#16
It’s important to keep in mind that achieving a lower A1c is not necessarily without a cost. And therefore you need to weigh the benefit and cost and see if the overall mortality risk is reduced.
For example, if you achieve a lower A1c by eating less carbs and eating more fat, while you reduce the risk of glycation, you may increase other risks from more fat, such as higher non-HDL lipoproteins, which increases ASCVD risk. Therefore, you’ve traded glycation for a different risk. Are you better off? Maybe, maybe not.
Studies show that both high fat diet and high carb diet increase mortality. The diet associated with the lowest all-cause mortality is somewhere in the middle: ~50% of calories coming from carbs. Again, it’s a U-shaped curve.
So if one tries to lower A1c, that’s great, but just make sure it doesn’t mess up other biomarkers.
2 Likes
Neo
#17
100% agree with you on this piece.
1 Like
This is when an SGLT2i such as empagliflozin or canagliflozin comes in. I’m thinking of adding it to my stack to reduce my HBA1C by 0.5, reduce my blood pressure, improve my cognitive functions, lose a few pounds, and increase my lifespan all for about $0.90 a day.
Why aren’t I taking empagliflozin right now? 
3 Likes
My last HbA1c from Jan 2024 came back at 5.0. That down from 5.5 in Nov 2023 and 5.8 in June 2023. I’m stunned really. That included all the sugary holiday feasts when I put on (and lost) weight. It was a test my doctor wanted related to my metformin prescription.
I’m not sure I believe it. But I’ll keep going with my program to see what another 3 months delivers.
2 Likes
LukeMV
#20
What does everyone think about using Fasting Insulin as an alternative for A1C?
1 Like
Dr. Green was fond of using HOMA-IR (which requires both glucose and insulin measurements). Sometimes a high HOMA-HR reading can be a predictor of future insulin resistance problems not yet showing up in the A1C.
3 Likes
I find HOMA-IR to be very useful - but the interesting thing is that is doesn’t correlate well with elevated HbA1C - at least not in my fit population. It will do much better in patients with significant obesity.
I have a lot of patients in their 60s-80s that are insulin sensitive, yet hyperglycemic.
4 Likes
LukeMV
#23
Good to know. I’m not obese, so I won’t waste my money on Homa-IR
1 Like
There are still people who aren’t obese that will see their insulin sensitivity go down and it is a warning sign long before developing T2DM. However, I see a lot of fit older individuals simply have a pancreas that doesn’t alert and decide to make much insulin until the blood sugar is higher.
The only added test need is a serum insulin level, which through labs I use is $12, that and a fasting glucose and run it through a free HOMA-IR calculator.
3 Likes
Note sur if HbA1c is that much a great number to look at, for example if you give blood a lot it can drop a lot, same if you’re anemic, or if your RBC live not enough time (bone marrow problem)