My insurers hate me. I’ve had 3 colonoscopies in 12 years with zero findings (I once said out loud that my mom has a polyp once). Now they’ve said not for 10 years. I think they meant I should just die.
5 Likes
Agetron
#130
Yes, that’s the problem.
The prices are all over the place.
Maybe they’re lowering some.There’s so much competition with cologuard. Insurance companies are pushing cologuard because it’s the cheaper route for your health check.
You are allowed to do cologuard once every 3 years. I was one of the earliest patients like number three hundred and fifty or so, and so I’ve actually had it done three times.
3 Likes
I had 2 where I woke up a lot during the procedure and one where I was out like a dead man. Must have been different drugs. Neither were a problem.
2 Likes
My insurance covers 92% of the cost for a colonoscopy in Hong Kong. Since they always find polyps, it’s never denied. It costs about 3000-5000 USD with anesthesia in Hong Kong, so about 240-400 USD after insurance with anesthesia. I need one every 2-3 years.
7 Likes
Wow. Congrats for dodging that bullet, @DeStrider !
5 Likes
Everyone should know that you can buy FIT tests OTC for US$22; their overall performance is about as good as the much more expensive first-gen Cologuard, and can be done as often as one wants.
6 Likes
sol
#135
Price is not the only difference.
FIT looks for traces of blood in stool. Because it only looks for blood, not DNA, there is a higher likelihood of false negatives than with Cologuard, which looks at both blood and DNA. (There will still be false negatives with both, of course.)
Me personally, I’m more concerned with false negatives than false positives, but false postives have their costs, too. What I found (2022 Harvard Health article) is that FIT has a false pos rate of ~5%, where Cologuard has a false pos rate of ~13%.
So there are trade-offs here. Comments from more knowledgeable folks welcome.
5 Likes
The U.S. Preventive Services Task Force recommends colon cancer screening and is more or less neutral on the method. FIT and the first generation Cologuard (“sDNA-FIT”) give similar performance overall. See their analysis of the benefits and harms of different methods in their systematic review and meta-analysis. And because FIT OTC is so cheap, you can do it as frequently as you like and/or layer it with other tests.
1 Like
Neo
#137
Are you talking about the new cologuard? The FDA has green lit an even better one.
No, I meant the first generation — I didn’t know the second gen had been approved. I’ll edit my second post accordingly.  Gen 2 is clearly better than Gen 1.
Gen 2 is clearly better than Gen 1.
1 Like
Neo
#139
@RapamycinCurious Actually my bad, next gen is not yet approved/available (but people seem to think it will be soon / for 2025).
1 Like
dankeen
#140
Even if it is only marginally effective then it worth doing multiple doses due to the low cost and risk and because it strengthens your immune system against multiple infections.
3 Likes
Novel Two Drug Approach for Tough-to-Treat Colorectal Cancer
A combination of two drugs can attack tumors in a non-conventional manner, according to researchers from the Netherlands Cancer Institute. Instead of inhibiting tumor cell division, this approach involves using one drug to hyperactivate oncogenic signaling to the point where cells become stressed. The second drug then attacks the stressed cells. The team suggests this may be a better approach for hard-to-treat cancers such as microsatellite stable colon cancer.
“Induced hyperactivation by Lixte’s PP2A inhibitor, LB-100, leads to hyperactivation of multiple oncogenic signaling pathways and acquired vulnerability to WEE1 inhibition,” senior author Rene Bernards told Inside Precision Medicine.
全文:Novel Two Drug Approach for Tough-to-Treat Colorectal Cancer | Inside Precision Medicine
2 Likes
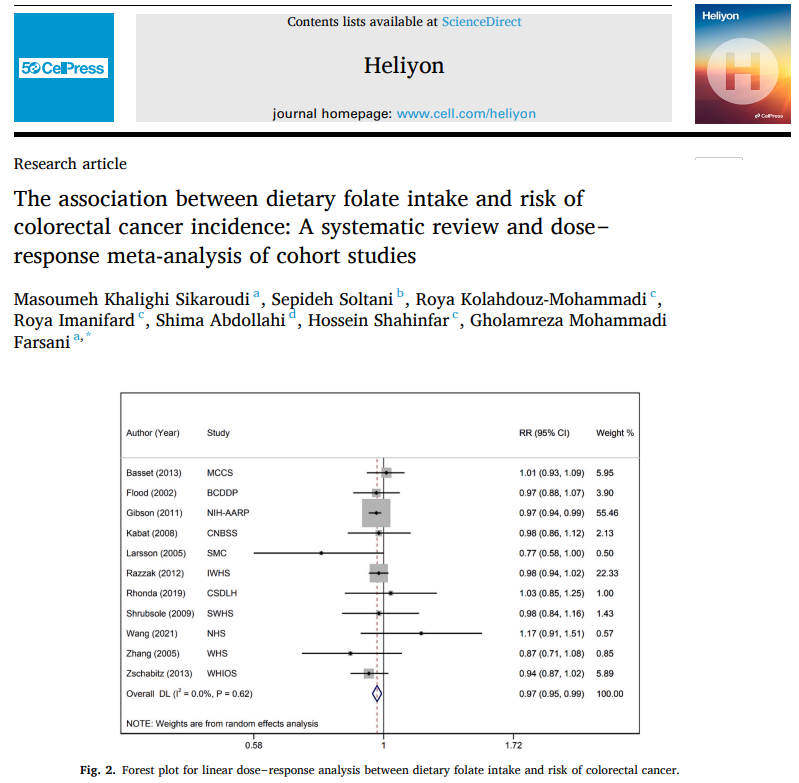
This systematic review and meta-analysis finds that a higher dietary folate intake is likely to be concomitant with a reduced risk of colorectal cancer, especially in at-risk individuals, and colon cancer, especially in females.
Open Access Paper:
The association between dietary folate intake and risk of colorectal cancer incidence: A systematic review and dose‒response meta-analysis of cohort studies (open access)
https://www.cell.com/heliyon/fulltext/S2405-8440(24)09595-1?_returnURL=https%3A%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS2405844024095951%3Fshowall%3Dtrue
1 Like
tananth
#144
I recently discovered a cancer blog which has numerous “treatment” protocols that consist of adding various off-label prescription or herbal supplements to standard-of-care cancer treatments (surgery, chemotherapy, radiation and immunotherapy) : https://www.cancertreatmentsresearch.com/summary-of-this-website/ and all protocols have supporting links to scientific paper and clinical studies. I have been skimming over the “treatment” protocols and was struck by how many of them could be used prophylactically as well, in line with the goals of this thread. In addition to Rapamycin there is:
-
Low Cholesterol slows cancer growth, but with a twist : what matters is the intra-cellular cholesterol (cancer cells require a lot of cholesterol for rapid cell division), NOT plasma LDL level. The best agents for lowering intra-cellular cholesterol are lipophilic Statins (like Atorvastin), Bempedoic Acid (which has independent anti-cancer benefits) and ezetimibe. PCKS9 inhibitors will not lower intra-cellular cholesterol and hence won’t help with cancer : in fact they may make it worse by increasing intra-cellular cholesterol levels. So if your LDL strategy is based on Statin + Bempedoic Acid + ezetimibe, you are also slowing down the growth of any cancer that has not yet been detected!
-
Well controlled blood sugar levels will slow cancer growth generally, but some anti-glycemic medications have additional anti-cancer benefits including Metformin (suppresses Mitochondrial respiration and fermentation, which slows cancer cells), Canagliflozin (a fermentation inhibitor with cancer suppression benefits NOT shared by other SGLT2 inhibitors).
-
Cancer tumors dump acid waste using Proton Pumps similar to the stomach lining and shutting down Proton Pumps systemically with Omeprazole + Cimetidine (both OTC in USA) and Telmisartan (and other ARBs used for blood pressure) can kill or weaken cancer cells. A lot of people take these on an ongoing basis, but probably didn’t realize they help prevent cancer.
-
Cancer tumors fend off the immune system by surrounding themselves with acid (low PH), which can be neutralized with Sodium bicarbonate or Sodium Citrate supplementation : this is safer long term than using Proton Pump inhibitors, so could be adopted by anyone even if they have no issues with acid stomach. Of course, if you have cancer, you should use both methods. In addition Citrate supplementation has an independent anti-cancer effect (beyond neutralizing acid).
-
Many common supplements that have been discussed here for anti-aging or general health also have anti-cancer benefits, including Tocotrienols (SREBP-1 & SREBP-2 inhibition), Honokiol (inhibits cholesterol storage), Aspirin, Berberine (Respiration inhibitor, similar to Metformin), Omega 3 oils, EGCG and Vitamin C (Fermentation inhibitors), Genistein (inhibits metastasis by making cells stick together, amongst many anti-cancer effects), Curcumin (multiple anti-cancer effects).
-
An old antihistamine called Cyproheptadine (OTC in most countries, but by prescription only in USA) is effective as a treatment against most meta-static cancers that stopped responding to chemotherapy, particularly against hard to treat Neuroendocrine cancers. It is prescribed 800K times per year in USA, often for hay fever (high pollen counts) and probably should be the preferred antihistamine agent for those worried about cancer, except that it has the negative side effect of weight gain (this is considered desirable for cancer patients and by some women in Africa where it is used chronically by young women in some countries).
12 Likes
Neo
#145
Can you explain how the medicines that are not statins have a big intra-cellular cholesterol impact outside of the blood circulation
A_User
#146
I wouldn’t be so sure about that. Atorvastatin has a lower incidence of diabetes compared to rosuvastatin, and if we speculate this could be off-target effects in muscles relating to HMGCR inhibition for the latter reducing the glucose sink.
1 Like
tananth
#147
I believe lipophilic Statins are better at penetrating the brain’s BBB, so would be better to control cancers in the brain. On the other hand, depleting cholesterol (particularly Desmosterol) in the brain can cause “brain fog”, which is less likely with non-lipophilic statins like rosuvastatin, though they still penetrate the BBB, just somewhat less. I would not use lipophilic statins just for brain cancer prevention if I had any symptoms of “brain fog”.
In the rest of the body there is probably no obvious difference between different statins in effect on intra-cellular cholesterol and hence no difference in effect on cancer prevention.
1 Like
A_User
#148
If you can measure serum desmosterol that is correlated with brain desmosterol.
I don’t think there is any recent evidence establishing the claim that some statins penetrate the BBB differently, if you have any I’d like to take a look at it.
If you can’t measure serum desmosterol then you cna use other things than statins.
1 Like