A_User
#13
Nope, it does not mean that.
5 Likes
Conspiracy beliefs regarding cholesterol will become the greatest filter in the quest for longevity. Maybe its for the best…
5 Likes
Bicep
#15
I think that will turn out to be the jab.
1 Like
No, no, no!  This is just too much fun and the new life extension news is quite scarce right now, mainly about new start-ups and researchers trying to get on the bandwagon and cash in.
This is just too much fun and the new life extension news is quite scarce right now, mainly about new start-ups and researchers trying to get on the bandwagon and cash in.
What I do is just ignore topics that I am tired of or not interested in.
4 Likes
I think the vast majority of doctors would disagree with you if you are saying statins are not beneficial and reduce CVD risk and all-cause mortality.
I am mystified by those who would ignore the preponderance of the evidence and instead choose to believe weak outlier studies.
The FraminghamHeart Study proved, as far as I am concerned, that high cholesterol, especially LDL cholesterol, increases heart disease risk. The Framingham study helped establish the role of cholesterol.
“The study began in 1948 and the participants have continued to be followed over the decades. By the late 1990s, the study had accumulated over 50,000 cohort-years of follow-up data. This large cohort followed long-term over many decades contributed to the landmark discoveries linking major cardiovascular risk factors like smoking, blood pressure, and cholesterol to heart disease outcomes.”
A similar large longitudinal cohort study in Denmark known as the Copenhagen City Heart Study. Initiated in 1976, the Copenhagen City Heart Study enrolled about 10,000 men and women aged 20-93 years old from Copenhagen. Participants were examined at baseline and followed for over 40 years, with several additional exams over time to update risk factor data."
And had virtually the same outcomes.
So are you saying that cholesterol control via statins has no significant benefits?
4 Likes
cl-user
#18
The issue is not cholesterol but the narrow minded simplistic focus on lowering LDL.
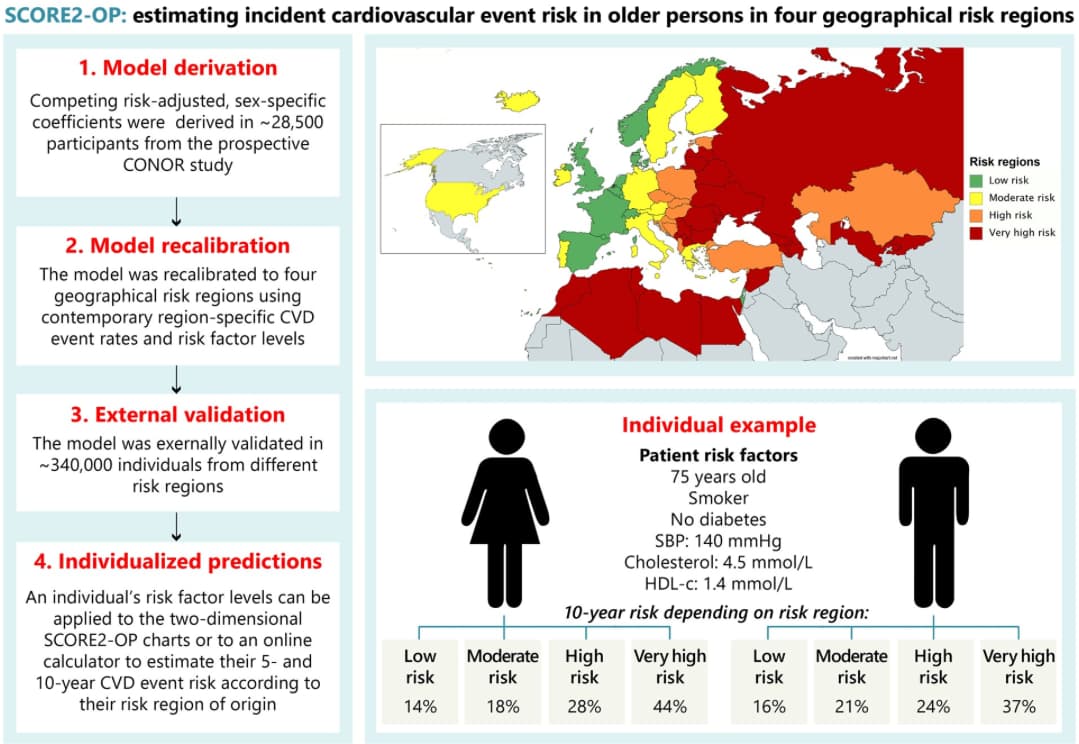
In the following post I used the official CVD 10 year risk calculator of the European Society of Cardiology and my LDL has doubled from 106 to 198mg/dl but my CVD risk is now lower.
The LabCorp NMR lipid panel also classifies me as low CVD risk.
None of those guys are cholesterol nor statin deniers BTW.
2 Likes
JuanDaw
#19
European and American cardiologists differ in their calculators. If you plug in your values in the American calculator.
https://static.heart.org/riskcalc/app/index.html#!/baseline-risk
Your risk is 7.1.
I made some assumptions you’re male (higher risk) and white.
The views on LDL may differ as well.
cl-user
#20
It’s because the US has a lower life expectancy than Europe.
I’m in the US but I’m French so I used the low risk region EU risk calculator.
Here are all the calculators for various EU countries.
That said that’s a huge risk increase for the US calculator.
Note that if I plug the values with the lower LDL in the US calculator, I get 6.7% which is basically almost identical.
1 Like
A_User
#21
You are missing the point so badly.
L_H
#23
I think you raise an interesting point. And I’m fascinated what people think of these statements all of which I happen to believe (but with varying degrees of confidence!). I think it might help tease out our biases.
- Apo b is a necessary factor in atherosclerosis
- Higher Blood pressure mechanistically increases the risk of apo b damaging blood vessel walls
- Statins have clear side effects for some people.
- Statins may have unclear side effects for others and so minimizing the necessary dose is sensible
- Statins have a clear net benefit in secondary prevention
- Statins have a population level net benefit in healthy 40+ year olds if taken for long enough
- Most of the apo b impact of statins can be replicated by lifestyle and nutrition
- We don’t know for sure what apo b to target, but it’s a lot lower than typical western diet population level, and is likely to be sub 70 mg/dl
- Apo b is not a sufficient cause of atherosclerosis
- Low inflammation or other factors may be protective against atherosclerosis in the presence of high apo b.
10 Likes
A_User
#24
Yeah! It’s totally a waste of time.
1 Like
tananth
#25
Though your LDL values are now higher (198 vs 106) your HDL values are also higher (95 vs 59) and higher HDL values can lower CVD risk more than a similar decrease in LDL. This is even more true for the ApoB and ApoA values. High ApoA (approximated by HDL) values, even seem to be able to reverse Atherosclerosis.
Any idea what you did to raise your HDL that high ?
1 Like
cl-user
#26
The change in cholesterol happened when I switched my diet to low carbs and started endurance training (running) at the same time 3 years ago. At the beginning, I went full Keto (basically no carbs) while running fasted in the morning to switch my metabolism to burning fats instead of carbs.
I have the Lean Mass Hyper Responder (MLHR) phenotype. That phenotype is defined by LDL 200+, HDL 80+ and TG < 70. Also my VHDL is too low to be measurable. The theory is that you need more cholesterol particles to transport the fats as a fuel but they are not atherogenic.
There is an ongoing study to see what the effect of those lipids is on plaque formation. The preliminary results are very good. LMHR people with an average LDL of 270 (but very high HDL and low TG) have less plaque than matched controls with low LDL. The subject with the highest LDL (500+) has no plaque at all.
1 Like
LaraPo
#27
What then contributes to plaque?
tananth
#28
The basic model is that inflammation (or injury) to blood vessels causes LDL to deposit plaque (as a kind of bandaid), but normally once the inflammation/injury resolves HDL dissolves the plaque and carries away the cholesterol from the plaque. In CVD, for some reason, the plaque becomes permanent and keeps growing.
1 Like
LukeMV
#29
I disagree. I enjoy reading smart posts and drawing my own conclusions on both sides. I used to live in a bubble and believe the “statins are poison and will kill you” crowd until I heard the other side which was much more evidence based. I wish I had been taking a statin from a young age instead of listened to them.
It seems clear statins have benefit but it’s over the long term, hence why this meta analysis doesn’t show a significant reduction in mortality risk. Atherosclerosis takes much longer than 3.7 years to manifest.
It just makes too much sense to start a low dose Rosuvastatin at a young age and then probably not have to worry about atherosclerosis much later in life.
Seems the negative studies have patients starting them way too late. Kind of silly to wait until you have a high calcium score to use one. Prevention is key.
5 Likes
cl-user
#30
Good summary. More info below.
If you have some time here is a long but comprehensive text about that:
The Role of Lipids and Lipoproteins in Atherosclerosis
Some excerpts in addition to @tananth 's summary:
Once LDL (APOB particles) enters a wall lesion, it has to be oxidized then that starts an inflammatory cascade. HDL is part of several mechanisms trying to fix that.
Surprisingly, native LDL […] has to be modified to promote foam cell formation. Oxidative modification converts LDL into atherogenic particles that initiate inflammatory responses. Uptake and accumulation of oxidatively modified LDL (oxLDL) by macrophages initiates a wide range of bioactivities that may drive development of atherosclerotic lesions.
The precise mechanisms that generate oxidized lipoproteins in vivo are still only partially understood. LDL circulating in the plasma appears to be protected from oxidation, both by dietary antioxidants such as vitamin E and C (259) and by protective enzymes including glutathione peroxidases […]
In contrast, an atheroprotective function of HDL is to prevent endothelial activation and enhance NO production to maintain barrier integrity
In addition, HDL maintains plaque stability by inhibiting degradation of the fibrous cap extracellular matrix through its anti-elastase activity
HDL, apoA-I, and endogenous apoE reduce lesion formation by preventing endothelial cell activation, inflammation, and oxidative stress and also by promoting cholesterol efflux from foam cells.
Again my point is not that statins are intrinsically bad but they are just one tool and that this is much more complex than the simplistic view of high LDL is bad and everybody should take them.
Not to forget that all the cause mortality as well as the centenarian studies show that a very low LDL is not optimal.
3 Likes
However, if you have high levels of LDL floating through your system and you happen upon an inflammatory event (which is hard to avoid 100% of the time) you may develop the plaque as your body treats the inflammation with calcification. Not an ideal situation, and very hard to avoid without maintaining low levels of inflammation (almost impossible) or LDL and ApoB (much easier with medication).
So, it’s much easier to go with treating LDL and ApoB than to make sure you never have an inflammatory event.
6 Likes
tananth
#32
While statin treatment to lower LDL seems to be the drug class with the greatest effect on lowering CVD, the anti-inflammatory Colchicine (discussed in other threads) reduces CVD by 31% (in those without CVD history), which beats all LDL lowering methods (other than statins), including PCSK9 
3 Likes
L_H
#33
Very interesting. What’s your personal supplement/pharma strategy? Do you try to focus on both ldl/apo b and inflammation? Or just inflammation and boosting hdl?
1 Like