Nick1
#101
I have been using redlight intermittently mostly face and hands. It is more than a coincidence that i get this itchy rash over face with onset of use. Previously I had attributed to Rapa. Rapa dose and regimen hasn’t changed However, during the off “biophotomodulation” period there is no rash. Has anyone experienced something similar? What’s the possible trigger?
Beth
#102
You are not crazy, Nick! I joined a red light facebook group and there are indeed people who don’t tolerate NIR and get a rash. Those people either turn off the NIR and just use red light on their faces, or they are farther away, or shorten the time.
1 Like
Seriously?
Bone is not metal, and red light does penetrate it.
DrT
#104
Hi DS,
If you have a look at this reference:
Henderson, T. Frontiers in Neurology 15, 1398894, (2024).
The author describes how they used lamb heads as a model to measure how much IR light reached down 3cm into brain tissue. Even with a 6 watt laser, only 0.01% was detected. With a 10 watt laser, 0.35% was detected.
A bank of 200 x 50 mw LEDs did not register at all.
He doesn’t dispute the beneficial effects of infrared light on brain injuries; but he disputes that it is a direct effect from penetration of the skull.
Yeah, it doesn’t look like there will be any significant penetration through most of the skull. Though the LEDs cited “Extensive prior research has shown that infrared light from a 0.5-watt LED will not penetrate the scalp and skull of a human.” are much weaker, 5 - 10 times than the ones used in quality panels, usually 2.5 - 5 watt LEDS.
The 800 - 900 nm wavelengths easily penetrate the eyeball so perhaps the face masks get a little into the brain. There are also some nasal LEDs" Nasal Red Light Therapy Device – FDA Registered’ that might get a little into the brain.
The inner walls of the orbit (toward the sinuses and nose) are among the thinnest bones in the skull, far thinner than the typical cranial vault bone.
Orbital walls (especially the medial and floor near the sinus):
Often “paper thin” – around 0.2–1 mm in places. These are much thinner than the calvarium (top of skull), often only ~1/5 to 1/10 the thickness of the parietal bone.
We must use methods, such as nasal, etc., where the bone is thin or provides a direct path to the human brain if we want to see any significant results.
I continue to use full-body RLT; if for nothing else, it feels good.
2 Likes
Beth
#106
Here ya go!
Spoiler alert, some gets through the scull.
Unfortunately, or fortunately, I will no longer be a good test subject to see if 1060 gives me relief from my concussion… my shipment was delayed and it’s only arriving today… my doc gave me propranolol yesterday and it completely wiped out all my symptoms (POOF!).
4 Likes
The TRUTH About Red Light Therapy for Skin and Hair - Is it Worth it?
AI Summary
Video Summary: Red Light Therapy for Hair & Skin (Dr. Dray)
A. Executive Summary
This analysis reviews the efficacy of photobiomodulation (red light therapy/LLLT) for dermatological and trichological applications. The core thesis is that red light therapy is a legitimate, evidence-based intervention for androgenetic alopecia (pattern hair loss), skin rejuvenation, and specific conditions like herpes labialis (cold sores). The mechanism relies on mitochondrial stimulation to boost cellular energy (ATP), thereby enhancing tissue repair and prolonging the anagen (growth) phase of hair follicles.
While effective, the therapy is not a “magic bullet” and is strictly dose-dependent; overuse can negate benefits. Success is contingent on consistency (daily or weekly adherence for 3–6 months) and using devices with verified power output (approx. 2500mW) and specific wavelengths (620–700nm). It is most effective when started during the early stages of hair thinning rather than on completely bald regions.
B. Bullet Summary
-
Mechanism of Action: Red light therapy works via photobiomodulation (PBM), where photons are absorbed by mitochondria to stimulate ATP production, energizing compromised cells.
-
Hair Loss Application: LLLT is effective for androgenetic alopecia (pattern baldness) by maintaining hair follicles in the anagen (growth) phase longer.
-
Efficacy Window: It is most effective for thinning hair; it cannot resurrect dead follicles in smooth, bald areas.
-
Skin Rejuvenation: Consistent use increases collagen density, improves elasticity, and reduces fine lines and wrinkle depth.
-
Herpes Treatment: PBM is an evidence-based treatment for cold sores (herpes labialis), accelerating healing and potentially increasing the interval between outbreaks.
-
Wound Healing: Red light accelerates wound healing and improves the final cosmetic appearance of scars.
-
Timeline for Results (Hair): Visible improvement in hair thickness and density typically requires 3 to 6 months of consistent use.
-
Timeline for Results (Skin): Skin texture and tone improvements generally appear after 6 to 12 weeks.
-
Dosing Sensitivity: Efficacy follows a biphasic dose response; more power or frequency is not better and can inhibit results.
-
Device Specs - Wavelength: Effective devices must utilize wavelengths in the therapeutic window of 620nm to 700nm (red) and near-infrared ranges.
-
Device Specs - Power: Adequate power output (e.g., 2500mW total output) is required to penetrate the scalp barrier; weak LEDs are ineffective.
-
Coverage: For hair loss, devices with high diode counts (e.g., 500 diodes) ensure consistent energy delivery across the entire scalp.
-
Safety Profile: The therapy is non-invasive and generally safe, but contraindicated for individuals with photosensitivity disorders or those on photosensitizing medications.
-
Synergy: LLLT can be combined with pharmacological treatments like Minoxidil or procedures like PRP (Platelet-Rich Plasma) for enhanced results.
-
Telogen Effluvium: While self-resolving, LLLT can support recovery from temporary shedding events (stress, marathon running, etc.).
D. Claims & Evidence Table
| Claim |
Evidence Provided |
Assessment |
| PBM increases ATP production |
Cited mechanism: Light absorption by mitochondria boosts cellular energy. |
Strong (Established biological mechanism). |
| Treats Androgenetic Alopecia |
Reference to multiple controlled trials showing improved hair counts/thickness vs. placebo. |
Strong (FDA-cleared indication; supported by meta-analyses). |
| Treats Herpes Labialis |
Stated as “one of the most evidence-based uses” for healing and preventing recurrence. |
Strong (Supported by peer-reviewed literature). |
| Reduces Hair Shedding |
Anecdotal personal experience + clinical indication for follicle stimulation. |
Strong (Consistent with LLLT mechanism on anagen phase extension). |
| More power/frequency is better |
Explicitly refuted: “Using it too frequently can jeopardize results.” |
Accurate (Adheres to the Arndt-Schultz Law of biphasic dose response). |
| Works on bald spots |
Refuted: “Works best for areas where you are noticing thinning as opposed to frankly bald.” |
Strong (LLLT requires a viable follicle to stimulate). |
E. Actionable Insights
-
Verify Wavelengths: Before purchasing, ensure the device emits light strictly within the 620nm–700nm (red) and near-infrared ranges. Avoid devices with “random” disco-light colors without specific therapeutic targets.
-
Check Power Density: Look for total power output metrics (e.g., ~2500mW for helmets). Low-power “wands” often lack the irradiance to penetrate to the hair follicle bulb.
-
Adhere to the Schedule: Do not exceed the recommended usage (usually 12–25 minutes every other day). Over-treatment triggers inhibitory effects (diminishing returns).
-
Commit to 3+ Months: Do not evaluate results before 90 days. Take baseline photos of the scalp/part line to track density objectively.
-
Combine Therapies: For aggressive hair loss, stack LLLT with Minoxidil (topical/oral) or Finasteride to attack the problem via multiple pathways (blood flow/ATP + DHT inhibition).
-
Screen for Photosensitivity: Review your current medication list (e.g., certain antibiotics, retinoids, diuretics) for photosensitivity warnings before starting treatment.
-
Treat Cold Sores Immediately: If you suffer from cold sores, apply red light at the “tingle” stage to potentially abort or shorten the outbreak duration.
H. Technical Deep-Dive
Mechanism: Photobiomodulation (PBM)
-
Chromophore Absorption: The primary acceptor of red and near-infrared light is Cytochrome C Oxidase (CCO), an enzyme sitting on the inner membrane of the mitochondria (Unit IV in the electron transport chain).
-
Nitric Oxide Dissociation: In stressed or hypoxic cells, Nitric Oxide (NO) binds to CCO, inhibiting cellular respiration. Red light photons dissociate NO from CCO, allowing oxygen to return, which restores the proton gradient.
-
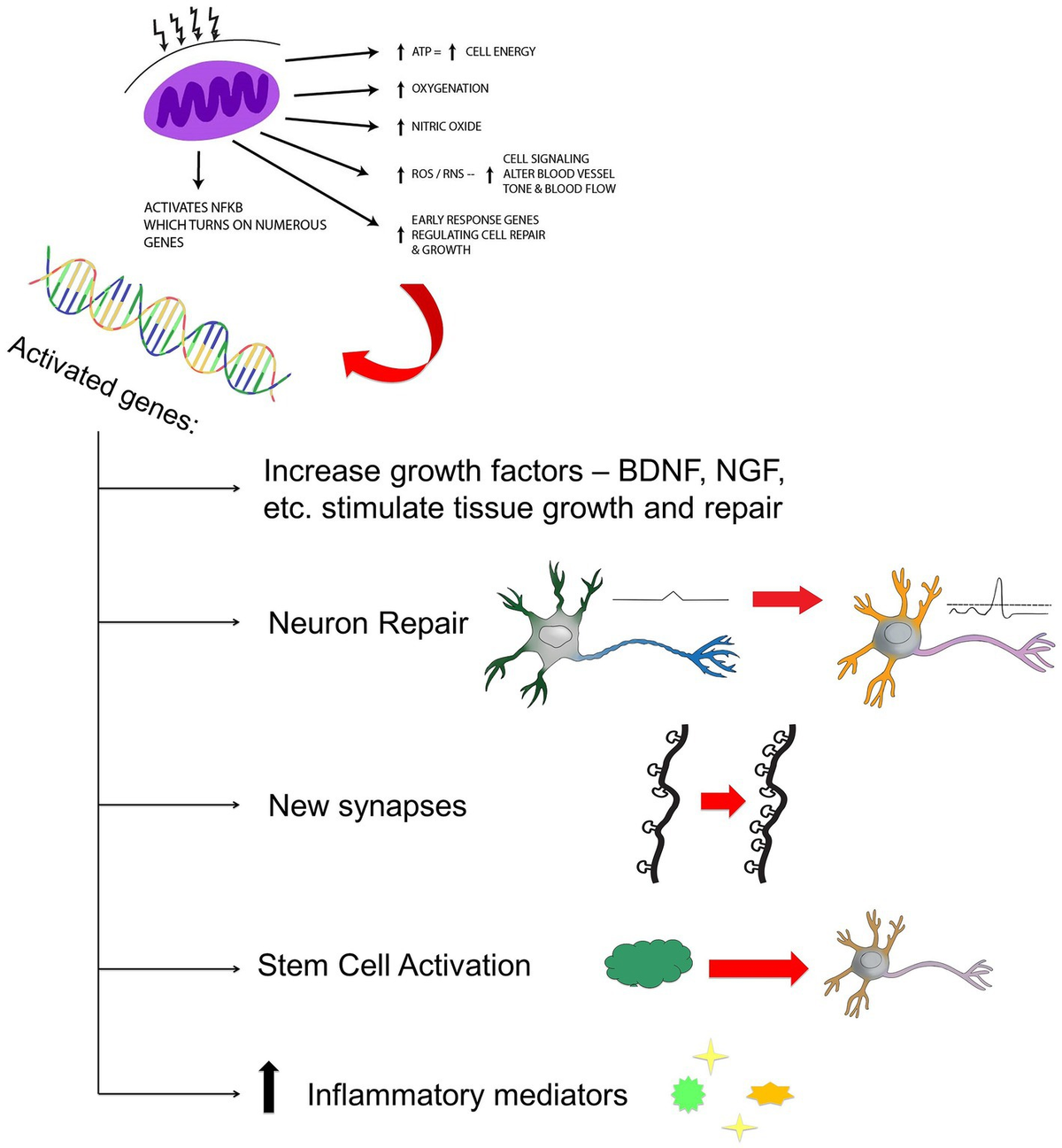
ATP Synthesis: The restoration of the electron transport chain leads to increased synthesis of Adenosine Triphosphate (ATP) and a transient increase in Reactive Oxygen Species (ROS), which acts as a signaling molecule to trigger gene transcription for repair and growth factors.
-
Biphasic Dose Response (Arndt-Schultz Law): Biological systems exhibit a non-linear response to light. Small doses stimulate; moderate doses optimize; large/excessive doses inhibit (cytotoxicity). This is why “more is not better” and adhering to the device’s timer is critical for mitochondrial health.
I. Fact-Check Important Claims
-
Claim: Red Light for Herpes Simplex (Cold Sores)
-
Consensus: Verified. Studies confirm PBM can reduce viral load and healing time. A 2013 randomized double-blind trial showed significant reduction in recurrence intervals.
-
Source: Invest Ophthalmol Vis Sci / PubMed.
-
Claim: Efficacy for Androgenetic Alopecia
-
Consensus: Verified. FDA clearance for LLLT devices for hair growth is based on safety and efficacy data. A 2014 meta-analysis found LLLT significantly increased hair density compared to sham devices.
-
Note: It is less effective than Finasteride (DHT blocker) but holds a superior safety profile (no systemic side effects).
-
Claim: Triple Wavelengths (625, 655, 680 nm)
-
Analysis: While valid, the exact combination of 625/655/680 is specific to the sponsor’s device (iRestore). The general scientific consensus supports a broader window (630–660nm and 810–850nm NIR). The specificity of “680nm” is less standard but falls within the therapeutic optical window.
3 Likes