A_User
#21
We already know the answer to the question that 30 LDL is better than 60 LDL…in clinical trials. So it is a false comparison.
Dr. Thomas Dayspring pointed out this article on Twitter today. The full article is available. Once again supporting the evidence that very low LDL is not harmful;
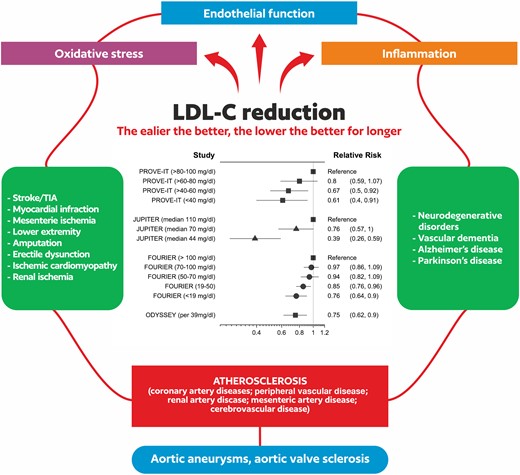
“There’s compelling evidence that atherosclerosis occurs only when LDL particles enter the intimal space, which initiates the inflammatory cascade that is atherosclerosis. If there are no LDL particles in the intima, atherogenesis does not occur.2 This requires keeping circulating LDL-cholesterol (LDL-C) levels low enough (the lower, the better), decreasing them early enough (the earlier, the better), and maintaining them throughout one’s lifetime (the longer, the better), which early detection and modern treatments can readily achieve in nearly every case.”
“Many facts suggest that a desirable, physiologic level of LDL cholesterol is far lower than previously assumed”
“All cells of the body make their own cholesterol”
“Those born with complete absence of proprotein convertase subtilisin kexin type 9 (PSCK9; loss of function mutation) suffer no ill consequences from lifelong near zero circulating LDL-C and have no atherosclerosis.”
“There seem to be no significant adverse problems from LDL no matter how low it gets. Recent randomized studies and meta-analyses have also shown that even very low LDL-C (<25 mg/dL, < 0.67 mmol/L) does not increase risk for dementia or haemorrhagic stroke”.
6 Likes
nym
#24
there is a caveat. people who have low levels of cholesterol production can be at risk for cognitive decline if their cholesterol levels are suppressed. Dr Dayspring acknowledges that. it’s about 20-25% population and you can get cholesterol dynamics measured thru Boston Heart. i’m in that population so did quite a bit of research. Unfortunately lipid trials don’t stratify by sterol phenotype so hard to know if benefits are across board or mostly in the majority of the population that has average cholesterol synthesis levels
2 Likes
Yes, you are right. Especially lowering LDL-C with statins is questionable in APOE4 carriers (gene that predisposes you to dementia, I guess 25% of population carry it). I posted a video in topic about dementia. Before taking statins as primary prevention (especially with normal levels of cholesterol) one should consider at least APOE4 testing and possibly desmosterol levels test to decide whether statins are best option.
4 Likes
David
#26
Thanks for sharing! In my population, it can be hard to get most people below 70 other than the truly motivated due to compliance of tolerating some of the higher doses of statins. Getting numbers as low as the 20s for LDL seems like a steep hill for the low risk population, but may be future.
2 Likes
jakexb
#27
Excellent podcast as always! I think this interview helped clarify for me where he is coming from. While he has become famous for his YouTube takes on various longevity topics, his philosophy on longevity is very much conservative and focusing on making sure everyone is taking care of those primary care basics of diet, exercise, sleep, blood pressure, cholesterol, stress… and his “extra credit” interventions are omega 3 and creatine.
And it’s a very sensible philosophy for a primary care doctor considering the vast majority of people are not even close to getting all the basics right, so basically even talking about the more exotic and less proven stuff that we talk about is not very sensible as a thing for him to focus on.
4 Likes
jakexb
#28
Wow, yea I’m on a statin and got my LDL down to 65 but… I don’t know what I would have to do to get it to 20. Definitely would have to throw some heavier drugs at it.
2 Likes
 Yes, I agree that he is conservative but not as conservative as the most physicians as you point out. It will be very interesting to follow how his approach develops throughout the years and see if he gets more open or more conservative.
Yes, I agree that he is conservative but not as conservative as the most physicians as you point out. It will be very interesting to follow how his approach develops throughout the years and see if he gets more open or more conservative.
By the way, what statin are you using and how do you combine it with your rapamycin intake?
1 Like
jakexb
#30
I’m on 10mg rosuvastatin. But also I’m currently taking a break from rapamycin… after I increased my dose from 2mg to 6mg, I started getting getting a ton of blood pressure related headaches and realized my bp was too high (140-150 systolic). I can’t be sure that the rapa was actually increasing the blood pressure or if it was coincidence, but I’m going to make sure my bp is stable for 6 months or so (taking losartan 100mg for that) before restarting my rapamycin, probably at a lower dose and tracking my bp.
It might not be connected, but this way I can isolate it as a factor as much as possible to see if there is an effect.
2 Likes