I look at CBC, Ferritin, how I feel, and once in a while, transferrin saturation (not dip below 20%). Ferritin dosen’t seem to be a very good metric for cellular iron stores, as I’m clinically “iron depleted” with Ferritin < 20. I’ve been donating regularly for 5 years, never any out of range CBC, no impact daily feeling, or on my daily exercise output. So clearly it would appear I’ve had excess iron in my body built up over a lifetime to 52 yo pre donations (57 now).
Your iron genes have a large impact on iron storage. I am homozygous H63D, so I would trend toward mild iron elevation. Maybe why my CBC is fine yet ferritin suggests otherwise.
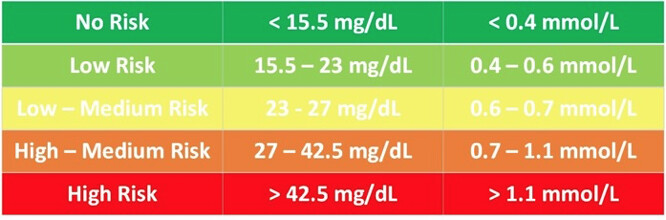
Some clinical benchmarks I watch for. I just want to skirt above deficiency which I have with regular 8 week donations.
As another check, I am tested for haemoglobin prior to every donation, I need to be above 125 g/L or I cannot donate.
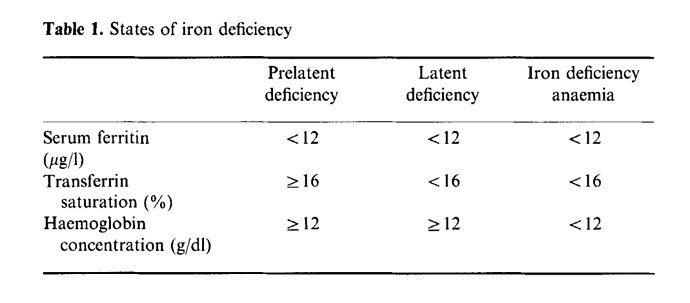
Iron depletion: serum ferritin less than 20 µgr/dl.
Lack of iron stores: serum ferritin less than 12 µgr/dl.
Iron Deficiency: serum ferritin less than 12 µgr/dl and transferrin saturation percentage less than 15.
Iron deficiency anemia: serum ferritin less than 12 µgr/dl, transferrin saturation percentage less than 15, and Hb less than 14 mg/dl.
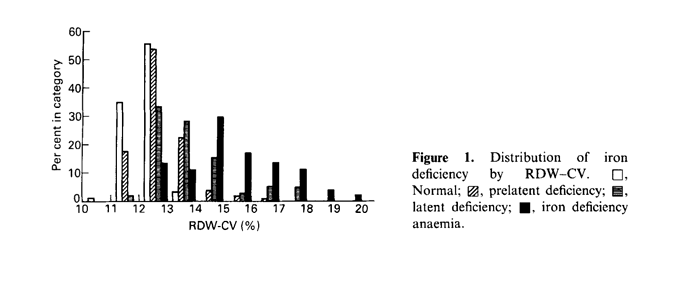
Here’s something very interesting…confounding? It appears that trending towards low iron leads to an increase in RDW, which in the Levine Phenoage calculator is a VERY heavily weighted parameter: the higher the RDW, the much older your phenoage.
So I am dumping iron/creating new albumin and generally “younging” my whole blood for longevity (plethora of literature supporting), yet Morgan Levine says I am aging and penalizing my biological age?
This appears to be a confounder in the classic U shaped curve epidemiological all cause mortality data? Sure hope so!
Change in red blood cell distribution width with iron deficiency
https://sci-hub.se/https://doi.org/10.1111/j.1365-2257.1989.tb00193.x
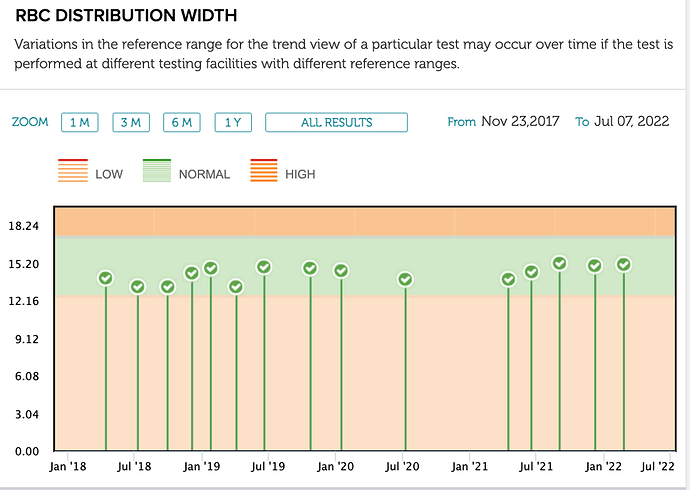
But my body so far seems to be tightly regulating my RDW, so not obviously penalizing me from a phenoage.