My latest last night was 99 SBP. Which is pretty low. 100-110 is my goal.
3 Likes
blsm
#588
You rock! I’m normally in the 90/60 range and feel good as long as it doesn’t drop lower. I don’t take bp meds.
2 Likes
Prav works for me. Went through a few before getting to Prav. My problem was always the leg pain so it made me “non compliant” LoL! I tried CoQ10 and it didn’t help with the leg pain initially but I stuck with that and continue with 100mg Co-Q10 today.
My low dose of 20mg Prav per day seems to be doing the job well enough with no side effects.
1 Like
LaraPo
#590
It’s great to have 90/60 without meds! It’s exactly what I had naturally before kidney transplant. Now it’s achievable only on meds unfortunately. I’m taking Nebivolol 1 mg, Amlodipine 5 mg, and Telmisartan 30 mg. Trying to reduce Nebivolol with a goal to eventually stop it.
4 Likes
blsm
#591
Thank you. I think you’re doing fantastic and in fact (not to be weird) I look up to you as an inspiration.
1 Like
LukeMV
#592
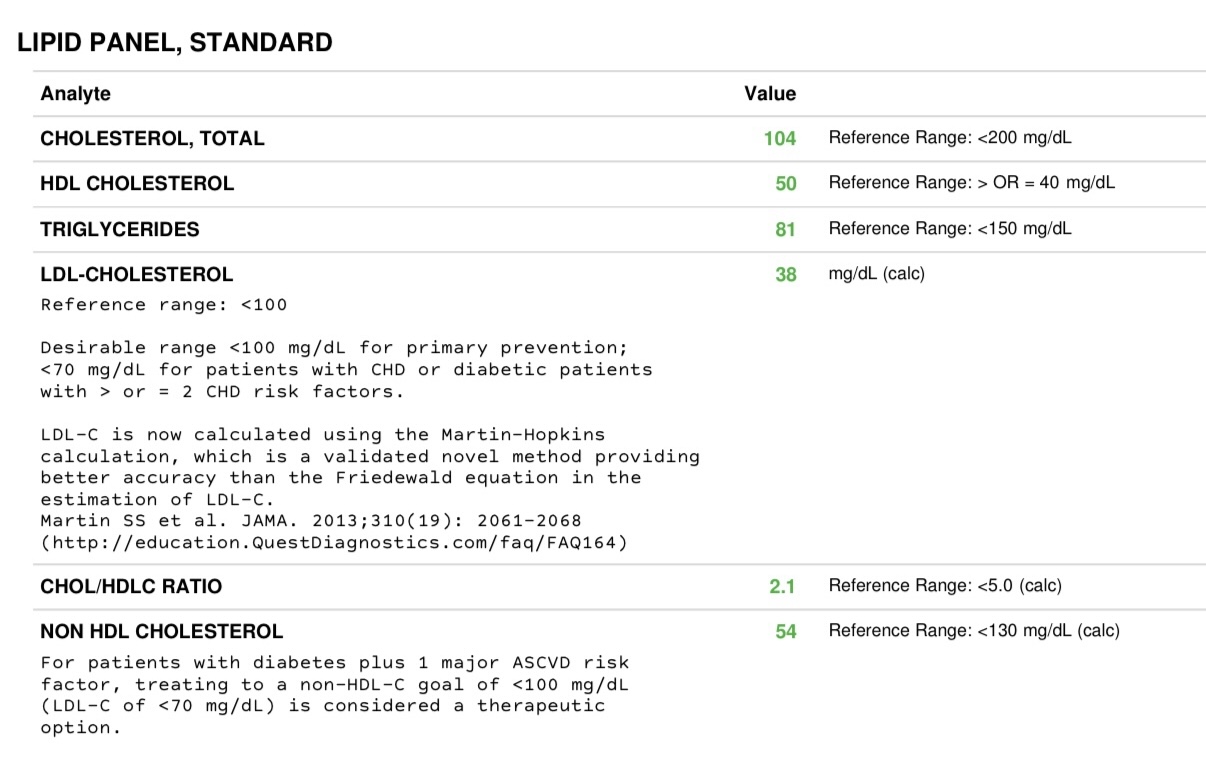
Just got a fresh lipid panel back. Obviously happy with this. 2.5mg rosuvastatin and 10mg ezetimibe are in play along with a high fiber diet. Also on 3mg Retatrutide which could be making things better as well.
I wasn’t even fasted so the triglycerides would probably be lower if I was
11 Likes
adssx
#593
Isolated Systolic Hypertension in the Young (ISHY) is common in tall and physically active males. In 2018 the EU guidelines concluded that if you NOT be treated with drugs in otherwise healthy people: Journal of Hypertension
However more recent papers show that ISHY is associated with a higher CVD risk:
But I might depend on whether you are otherwise healthy or unhealthy: Isolated systolic hypertension in young males: a scoping review | Clinical Hypertension
Conclusion:
- As others said, repeat the measures and exclude white coat hypertension.
- If normal diastolic and ISHY is confirmed then first look at lifestyle (diet, sleep, exercise, weight loss, etc.) but if your 15yo is a tall healthy physically active male then it’s unclear if there’s anything to do

4 Likes
Nice going! Your triglycerides are already at a good value and I doubt your apoB is affected by it.
I myself am currently experimenting with pravastatin 10-20mg (recommended by Dr Stanfield) and tirzepatide 7.5mg since I had elevated liver values with pitavastatin (no muscle issues). If I don’t manage to consistedly get below 60mg/dL LDL-C I will add ezetimibe. My lp(A) value is luckily extremely low but due to high stress levels and insomnia I want to drive cholesterol levels down further.
3 Likes
LukeMV
#595
Yep my ApoB has always been similar to my LDL (maybe a tad higher) and my Lp(a) is low (thank god) so I didn’t ask for them this time.
1 Like
I thought I’d share a brief experience report. I’ve been taking Telmisartan 160mg for a few months now and my at home measurements have seen no change - 115/75 before and after. Interestingly, my in-office BP has been consistently lower - upwards of 135/95 before and now 110/70 or even lower. I don’t have a good explanation for the discrepancy, I always assumed it was just white coat anxiety, or bad testing setup. Either way this seems like a positive result.
I’m primarily taking it for PPAR activation, so any BP or BPV lowering effect would’ve been just a bonus for me.
3 Likes
LukeMV
#597
I’d be interested to know your potassium level next time you get lab tests at that dose
1 Like
How do you assess your BP? At home, have you used an ambulatory monitor or a standard seated readings? I ask, because when there are differences between BP readings at the doctor’s office and at home, it is useful to do 24 hour ambulatory readings to pinpoint whether it’s an isolated white coat effect or if your BP regularly spikes and you are simply not capturing it in seated readings at the times you happen to take your measurements. In particular it can be of interest what your BP is at night when you’re asleep, because obviously you are not taking seated measurements at that time, whereas nighttime BP is very meaningful in assessing health.
2 Likes
Standard seated, though at various times during the day. I have a Whoop that promises overnight readings, though it’s unclear to me how accurate/validated it is (and I haven’t set it up yet). Will get a Aktiia/Hilo once it’s released in the US
Thanks. FWIW, there’s also this: CONTEC ABPM50 24 Hours Ambulatory Blood Pressure Patient Monitor, on Amazon, Ebay etc. - I bought it a few months ago, and am embarrased to admit, have not opened the box as yet.
2 Likes
Association between blood pressure trajectories and high carotid intima-media thickness in Chinese children
Cardiovascular diseases (CVDs) is the leading cause of morbidity and mortality worldwide [1], and identifying early cardiovascular risk factors is essential for primary prevention. Hypertension is a well-documented risk factor for the development of CVDs in adults, but recent evidence suggests that cardiovascular risk may begin in childhood [2]. Findings from longitudinal cohort studies investigating the trajectory of blood pressure (BP) showed that individuals with high BP in childhood are more likely to maintain high BP in adulthood [3].
Carotid intima-media thickness (cIMT), a recognized surrogate marker of atherosclerosis, is highly predictive of future cardiovascular events. The thickness of the intima-media layer of carotid arteries has been found to increase with age, which is influenced by CVDs risk factors, including elevated BP [4]. A growing body of literature indicate that high BP is associated with increased cIMT during childhood 5, 6, 7. Prior investigations have relied on cross-sectional assessments of BP to estimate associations with high cIMT, neglecting the temporal dynamics of BP fluctuations across critical developmental periods. Moreover, the field has concentrated almost exclusively on adult cohorts, resulting in a paucity of evidence regarding whether childhood BP trajectories predict CVDs progression into young adulthood.
Discussions
In this cohort study of Chinese children, we identified three distinct trajectory groups for both SBP and DBP from childhood to adolescence. Furthermore, we observed a significant association between SBP trajectories and the increased odds of high cIMT.
We found that the odds of high cIMT were significantly higher in children from ‘mid SBP’ or ‘high SBP’ trajectory group than those in the ‘low SBP’ trajectory group.
Paywalled paper:
https://www.sciencedirect.com/science/article/abs/pii/S0939475325004120
Potassium 4.3 mmol/L, range 3.5 - 5.2 on 08/04. My range over the past 2 years excluding this draw is 4.4 - 5.2, more typically in the 4.4-4.6 range.
1 Like
Telmisartan appears to have raised my Adiponectin modestly, in line with the literature, latest result is 5.5, following my previous two results of 2.2 and 3.9 (without Telmisartan). I would like to see it a bit higher so I’m considering dropping to 80mg, re-testing to see if there’s any difference, and then possibly adding a low dose of pioglitazone, say 7.5mg.
5 Likes
Reasonable approach. Pioglitazone might also lower BP very slightly.
adssx
#606
Updated American guidelines: https://www.ahajournals.org/doi/10.1161/HYP.0000000000000249
One big difference: treatment is now recommended to anyone above 130/80 mmHg “after an initial 3- to 6-month trial of lifestyle modification” (diet, exercise, etc.). Goal is “<130 mm Hg, with encouragement to achieve SBP <120 mm Hg”
5 Likes