Josh
#121
I’m going to try nebula as well. Any tips on how to utilize results for health advancement?
hamtaro
#122
It was a couple years ago, but I remember it took a bit of trial and error. I think I also got the invalid header with the VCF file. But ultimately, I believe I downloaded the whole cram file. I remember downloading a very large file, I think it was something like 40gb, but not 100% sure. I might have zipped it before uploading… sorry, I don’t have a copy of that file… probably because it was so large.
2 Likes
hamtaro
#123
Nebula comes with its own system of evaluation, but Promethease is the best way to fully take advantage of it. Once its in promithease, it works just like the smaller dataset from 23andme/ancestry. You can just filter the set based upon topics, conditions, diseases, etc.
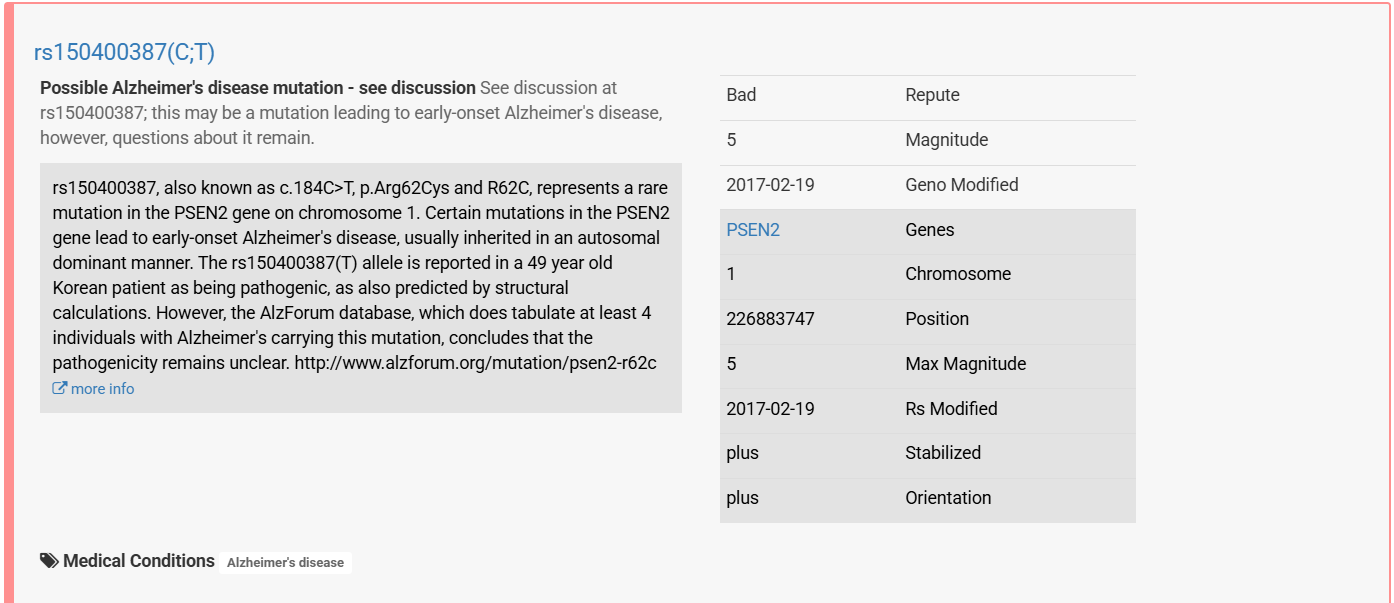
It lists the genes by ‘magnitude’. APOE4 is a 3, 9p21 is a 4, and what I got was a 5. But I quickly read that it was very rare, not very well-studied, and assuming it behaved like other PSEN2, it would cause AD in almost every person who had it, by the time they are 50. However, after researching it in more depth, I found out that it was ‘Autosomal Dominant’ so it would’ve had to have come from one of my parents; neither of whom had AD. One made it to 80, the other is still alive at 82. I also found a reference to it from a researcher, who said it likely had no effect. I’ve attached the info for viewing:
4 Likes
Josh
#124
This seems to have a good 2023 overview of choline supplements and risks with a dedicated section on cognitive dysfunction. "a lifelong choline supplementation may have beneficial cognitive effects such as decreasing amyloid-β plaque load and improving spatial memory in the APP/PS1 mouse model of Alzheimer’s disease…In another paper, the same group reported that maternal choline supplementation has profound benefits in Alzheimer’s disease pathology by reducing brain homocysteine levels across multiple generations "
A cross-sectional study conducted on ~2400 elderly patients demonstrated that choline intake, defined as the combination of dietary and supplement intake, correlates with cognitive performance (151). Choline supplements in the form of lecithin and choline chloride did not significantly improve memory performance in humans although some papers have reported positive outcomes in cognitive function of animal models (152–156). However, other choline supplements such as citicoline, choline bitartrate, and GPC appear to be very promising in the treatment of elderly patients suffering from dementia.
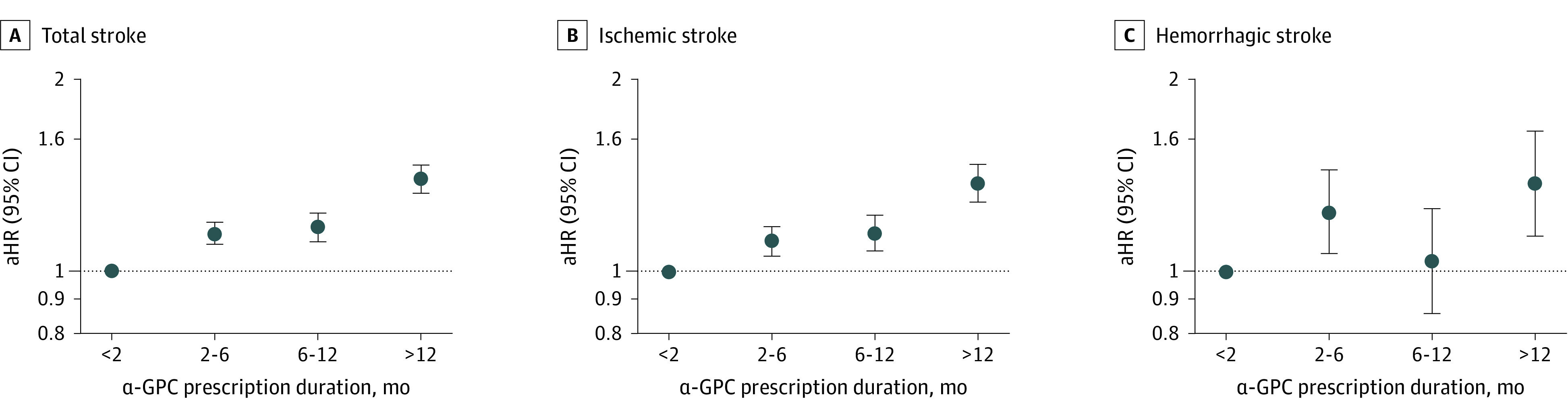
Paper does point out a concerning risk of stroke increase from lifelong alpha GPC supplementation. Maybe from raising TMAO and gut microbe changes? Choline bipartate probably raises TMAO more than the others because it is less absorbed (and has links to kidney stones made of calcium tartrate tetrahydrate).
tldr take citicoline and alpha GPC for dementia
6 Likes
Josh
#125
It appears no risk for a-GPC strokes for use under 2 months. I cannot find what prescription dosage is, but AI seems to think it is 400mg 3x a day which is far above what I would want - probably more like 200-500mg a day.
So I will probably rotate it weekly with citocholine and keep monitoring my TMAO levels occasionally.
1 Like
Rapan
#126
This is an alternative to Promethease.
It’s free and worked with the VCF from Nebula.
https://geneticgenie.org/
I am still working on Promethease. Cram doesn’t seem to be accepted too. I am in the process to convert the data fron Nebula, but there seems to be a problem about false positive results with Promethease when using the converted file.
4 Likes
I take 500 mg daily in the morning.
2 Likes
@Rapan Thanks. Says I clear rosuvastatin slowly (high AUC). Maybe that’s why I had a problem with it. (But I don’t think the issue is limited to rosuvastatin as I had a worse problem with atorvastatin).
hamtaro
#129
Nothing really new here. He just highlights a study that revisited the SPRINT study. But he does a nice review. In short:
Keep SBP below 120
reduce salt, increase potassium, dash diet
exercise snacks, wall squats
control weight
Consider medication if all else fails
He does focus on the cumulative effect of having high blood pressure for decades, and how it can have an absolutely catastrophic effect on cognition.
7 Likes
Have you tried Alpha GPC? Appreciate @Josh comment on this.
This article is very interesting. Basically indicating that for adults currently over age 55 years, lifetime risk of dementia is 42% currently. Frequencies of ApoE alleles are as follows:
ApoE4/E4 2-3%, Heterozygous for ApoE4 (e.g. one E2 or E3) is 22%, and 59% have ApoE3/E3.
So 25% of people have and ApoE4 (or 2) and yes, more risk of dementia. Currently 40-65% of patients with AD have at least one copy of an ApoE4.
3 Likes
Karina52
#131
definitely no galantamine. Lots of side effects and no benefit. I’m 72 yr old APOE4 homozygote and my prevention protocol is rapamycin (was patient of Dr. Green), a-Klotho protein, lipid replacement therapy (Prodrome Plasmalogens) to optimize brain fats, hormone replacement therapy including pregnenolone, DHEA, BHRT. High dose melatonin, Red light therapy, NAD, B12 shots, amino acids, peptides and more. When I go quietly into that good night, I plan to take all of my marbles (and memories) with me!
8 Likes
Could you share your rationale for this target range in ApoE4 patients?
1 Like
DrFraser
#133
Good question, and I’ve not dug up the studies. When I recently completed my Cardiovascular Fellowship module with Dr. Mark Houston who is a great cardiologist, and runs one of a few similar centers in the U.S., in Nashville, his recommendation is everyone with cardiovascular disease should be running Vitamin D’s 70-90 ng/mL (nl 30-100 ng/mL). I haven’t looked up the details on every item I was taught in the fellowship module.
I haven’t dug up the papers he uses to support this is the syllabus. On a quick AI review … I wish it would give the citations, here is what was concluded separately with CV disease and Neurocognitive decline. As the 2 are linked, I’d rather take the more aggressive dosing.
Optimal Levels: While studies have not definitively determined the “perfect” level for cardiovascular health, maintaining serum vitamin D levels within the range of 20–40 ng/mL (50–100 nmol/L) is often recommended for overall health, including heart health. Some studies suggest that levels on the higher end of this range may be particularly beneficial for reducing cardiovascular risk, but too high a level (over 100 ng/mL or 250 nmol/L) can cause toxicity and might increase risks, including calcification of blood vessels.
Optimal Levels for Brain Health: While the optimal level for neurocognition isn’t universally agreed upon, maintaining a level within the 20–40 ng/mL range (50–100 nmol/L) seems to be beneficial for general cognitive health. Some studies suggest that levels closer to the higher end of this range (e.g., 40–60 ng/mL) may provide neuroprotective effects, particularly for people at risk of cognitive decline or in older adults.
4 Likes
59vw
#135
Maybe I missed it (that’s a long list!) but I’d add KLVS testing to your genetic testing items. KLVS variant is relatively common (~25% in the US) and almost converts an APOE 3/4 to an APOE 3/3 risk status.
Find me a company that does this test. I cannot, and also would the actions be any different than the rest of the advice given? I can’t think of anything beyond that would impact this apart from direct supplementation of Klotho, which at current prices would be $400/day to get a similar amount to the monkey studies.
2 Likes
59vw
#137
Find me a company that does this test.
would the actions be any different than the rest of the advice given?
Information can be powerful therapy (perhaps even better than Rapa!) You could make the same argument for sequencing PSN1 and PSN2 and APP. In fact I’d suggest you not sequence these genes unless your patient has a family history of early onset AD. The reason being is you will get any number of variants of uncertain significance that will produce a lot of anxiety that you can do nothing about and most are unlikely disease causing variants.
KLVS is common (~25% of population) and is a welcome piece of information reducing risk of AD. Pair that with APOE4/4 genotypes and it is huge to know whether you are KLVS het or not. I agree supplementing with klotho is not economical and not safe using the current distributors but looking at KLVS status is the same logic as looking at APOE4 status in the first place.
Most people reading this forum are interested enough in genetic predisposition that they should have their genome sequenced rather than dabble with the costs of sequencing individual genes or genotyping companies like 23andMe. Whole genome sequencing is available commercially for less than $1000 including analysis and Nebula (https://nebula.org/) will do it at 30x coverage for $195! I personally like George Chruch’s company Veritas. https://www.nanalyze.com/2021/07/whole-genome-sequencing-precision-health/ This is different than genotyping that is provided by companies like 23andMe.
WGS has multiple benefits of providing non-coding regulatory sequences and introns (which often identify splicing mutations). I’ll admit I did my (and my wife’s) genomes myself in my lab so I don’t have experience with ordering this commercially but it seems straightforward. I have my genome alignments in BAM format on my computer and can look up every new scientific finding as they are published. There is free software (I use IGV developed at MIT) to view sequence variants.
4 Likes
Josh
#138
I think 40 to 60 is optimal and rhonda pattrick agrees. She point’s out risk above 60. She says the science is not settled on optimal.
Consumer labs is even more conservative and says dont go over 40ng or 4000 iu. Petter attia takes 5000iu which is what i do and it puts me just above 40. It seems taking 10k iu is considered risky long term.
DrFraser
#139
Monitoring blood levels with taking Vitamin K2 MK7 I’ve not seen a single case of hypercalcemia. It’s not until we get over 100 that we get into issues with this. Just my 30 years of clinical experience. Appreciate the PhD who doesn’t have a medical license and her opinion and selecting some literature, but as someone who treats patients, sees response to therapy and sees their labs … I’m pretty happy with the approach of pushing the levels to 70-90 especially in those with CAD or risk of neurocognitive disease. I’ll go with Dr. Mark Houston over Rhonda Patrick any day on this issue.
Also the units/day and putting limits on this without monitoring makes little sense. Take a look at Target D where there is individualized response to therapy with 15% needing >10,000 IU/day in order to just get to 40 ng/mL. So absolute numbers on dosing shouldn’t be the recommendation unless blood tests are not possible.
I do usually start people who are not optimal on 5000 IU/day with at least 200 mcg of Vitamin K2 MK7, but then we check the results 3 months later.
11 Likes
Josh
#140
I do appreciate that study with how hard it is for some people to raise their vitamin D levels. I can’t find anything written by Dr Houston? Does he have any articles about Vitamin D? I found this but the link doesn’t work, but seems to recommend 60:
I found one 3rd party site saying Dr Attia also recommends 40-60, but couldn’t find a number on his site.
LifeForce physicians recommend 50-100 as optimal.
1 Like


")