Intranasal and inhaled delivery systems for targeting circadian dysfunction in neurodegenerative disorders, perspective and future outlook 2025
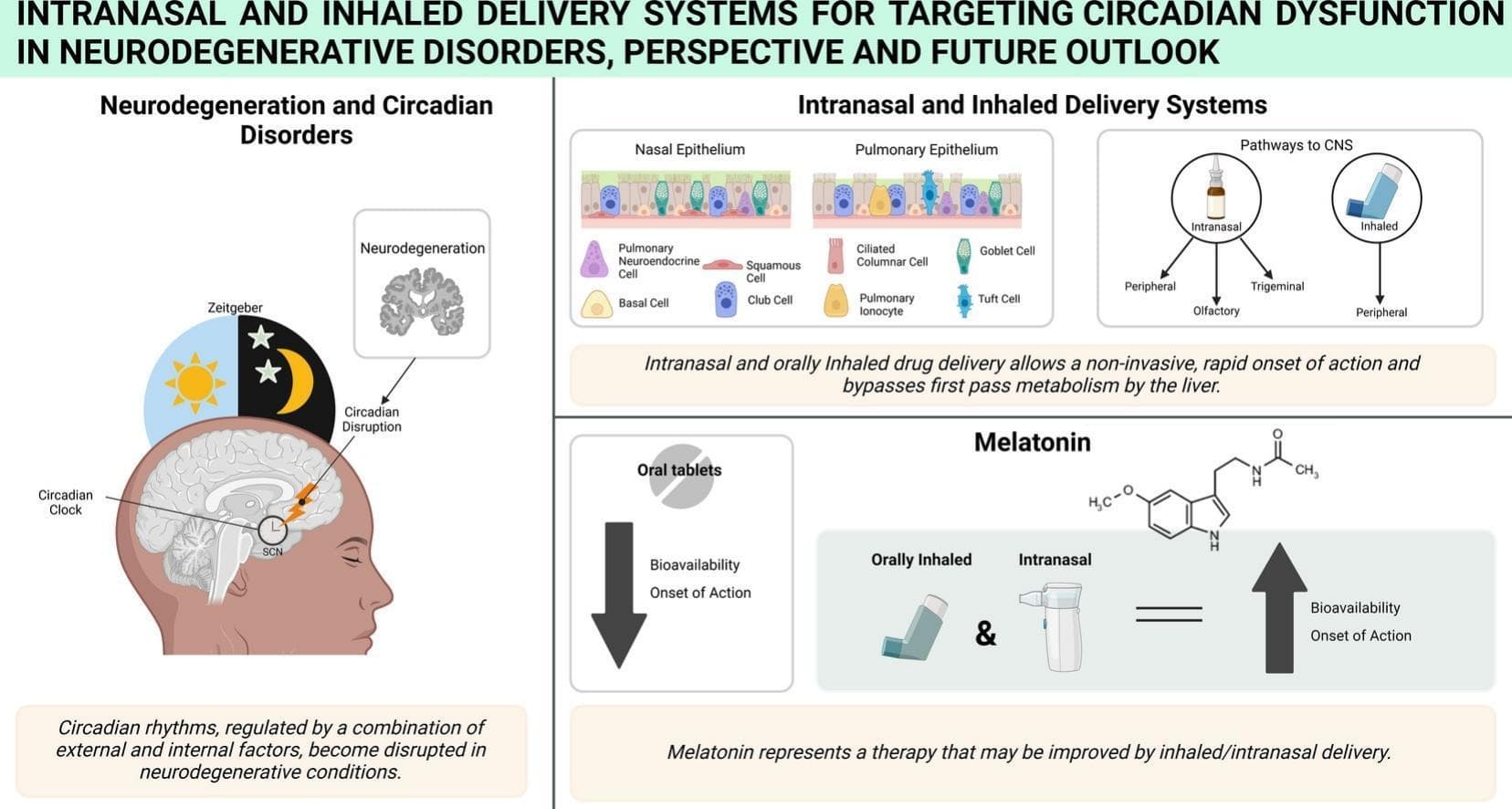
Oral medications often face challenges in achieving the necessary systemic circulation to effectively bypass the blood brain barrier (BBB) and reach the CNS, primarily due to low or variable bioavailability. Advancements in non-invasive delivery methods, such as orally inhaled and intranasal formulations, present promising alternatives for targeting the CNS. Orally inhaled and intranasal drug delivery allows for medications to rapidly achieve high systemic circulation through increased bioavailability and fast onset of action. Additionally, intranasal delivery allows for therapies to bypass the BBB through the olfactory or trigeminal nerve pathways to directly enter the CNS. This review assesses the potential for orally inhaled and intranasal therapies to treat circadian disorders in neurodegenerative conditions. In addition, this review will explore melatonin as an example of enhancing therapeutic outcomes by adopting inhaled or intranasal drug delivery formulations to improve drug absorption and target circadian disorder more effectively.
Despite its widespread use, oral melatonin has limited bioavailability, typically around 15 %, due to poor absorption from the gastrointestinal tract or extensive first-pass metabolism in the liver. Bioavailability also varies greatly between individuals, influenced by factors such as gender, caffeine and smoking, oral contraceptive use, age and the co-administration of fluvoxamine. In addition, pharmacokinetic studies have shown substantial variability in the time to reach maximal concentration (Tmax) following oral administration. Rapid release formulations have been found to range from 46 to 90 min with doses of 2 and 25 mg, respectively. Two different 10 mg oral extended-release formulations, from the same study, demonstrated Tmax values of 45 and 210 min. The variability in patient melatonin uptake may limit the effectiveness of oral melatonin as a therapy and could hinder research into oral melatonin formulations.
Although not currently commercially available, intranasal melatonin was first examined in 1981, whereby a small placebo-controlled crossover study of healthy adults (n = 10) reported that an intranasal dose of 1.7 mg of melatonin could effectively induce sleep.
Merkus and colleagues reported a Tmax of 5 min for intranasal melatonin administration (compared to 10 min for intravenous) in a crossover study of three individuals.
While intranasal administration demonstrates promising bioavailability and therapeutic potential, given melatonin readily passes the BBB and accumulates in the CNS at higher levels than in the blood, there may be a more straightforward route for delivering melatonin to the brain—via oral inhalation. Orally inhaled melatonin delivery could offer a direct path to the CNS while avoiding the drawbacks of intranasal delivery, such as limited dose size or reduced absorptive surface area of the nasal mucosa compared to that of the lung.
Given the absence of human studies on inhaled melatonin, a recent modelling study showed the pharmacokinetics of inhaled melatonin, demonstrating that a 2 mg dose of inhaled melatonin would reach a theoretical maximal plasma concentration (Cmax) 26.8 times higher than that of a 2 mg oral dose of melatonin. Furthermore, the theoretical Tmax of inhaled and orally delivered melatonin were found to be 0.2 min and 35.6 min, respectively, demonstrating that inhaled melatonin could provide a considerable improvement in the onset of action, thus, assisting with the management of circadian disorders.
Despite the scarcity of information to verify the safety and efficacy of delivering melatonin via oral inhalation, several ‘vape’ and ‘diffuser’ e-cigarette products, containing highly variable dosages of melatonin, have become commercially available; often marketed as sleep aids
The popularity of melatonin e-cigarettes can be inferred from a recent cross-sectional study of United States residents that found that over a quarter of their 6131 participants (56.3 % female; 43.7 % male; mean age 21.9 years) reported using melatonin vapes
To help address the gap in the literature surrounding the efficacy and safety of inhaled melatonin, the authors of this review have recently registered randomised open-label crossover human clinical trials comparing the effects of an orally inhaled formulation of melatonin delivered by MDI against oral melatonin tablets (CTR No. NCT06802913 & NCT06801379). These trials aim to investigate the pharmacokinetic profile of melatonin delivered by orally inhaled administration, as well as examine the effect on sleep architecture measured by overnight polysomnography in older adults with insomnia disorder. A validated air–liquid interface model of the alveolar epithelial layer [130] was used to gather currently unpublished, preliminary data examining the safety of depositing inhaled melatonin within the lung periphery. Thus far, both the trans-epithelial electrical resistance and the apparent permeability (measured by sodium fluorescein assay) of air–liquid interface models have not indicated that inhaled melatonin delivery compromises epithelial integrity, suggesting it will be well tolerated by the human lung.
Did you know about melatonin e-cigarettes @John_Hemming?