Just looking more at these drugs… Hydoxyzine is another anticholigenergic drug, so again the same side effects as meclizine.
The other two drugs however are not on the list so may not have the same side effect issues:
Common side effects
These common side effects happen in more than 1 in 100 people.
Talk to your pharmacist or doctor if the side effects bother you or do not go away:
- feeling sleepy during the daytime
- feeling sick
- indigestion
- putting on weigh
Flunarizine
Who should not take flunarizine?
People with the following conditions should discuss taking flunarizine with their doctor.
- hypersensitivity to flunarizine or any of its ingredients
-
depression or previous episodes of serious depression
- Parkinson’s disease or a family history of Parkinson’s disease
- liver damage
What are the side effects of flunarizine?
The main side effects of flunarizine are tiredness, drowsiness, weight gain and low mood.
- Tiredness and drowsiness can be reduced by starting with a low dose and taking it at night. The dose will then be increased gradually once your child becomes tolerant to these effects. Some patients experience a second wave of tiredness after several weeks or months and it would be advisable to either try a lower dose or use the medicine on alternate days. This should be discussed with your doctor
- Possible weight gain is caused by an increase in appetite and can be avoided by your child following his or her usual diet without any increase in portion size. In our experience, this happens in one in ten children taking the medicine.
- If your child develops low mood or depressive symptoms, the medicine should be discontinued. You should take advice from your family doctor (GP) whether specific treatment may be necessary for the treatment of depression if the symptoms do not disappear within one month.
There have also been reported cases of flunarizine causing symptoms as seen in Parkinsons’s Disease (extrapyramidal symptoms) which usually disappear when flunarizine is stopped. Other side effects that have been reported include: sickness and upset stomach, insomnia, dry mouth, weakness and muscles aches, and a skin rash. If you are concerned about any of these, please tell your doctor.
1 Like
Cinnarazine would be worse since one of its side effects involves the extrapyramidal reaction of tardive dyskinesia. Sometimes irreversible and caused by depleting dopamine.
Not good especially in the elderly.
2 Likes
Same idea with flunarizine. Extrapyramidal reactions are more common in the elderly and tardive dyskinesia can be life changing in a bad way. It’s the main reason that an entire class of antipsychotics has been replaced by the atypicals.
1 Like
It sounds like its rare, and reversible…
RPS
#43
Fair enough - how is the level of calcium in your diet (I’m assuming your vitamin D and K are at good levels)?
Incidentally, although you are feeling underwhelmed with Rapa, you have mentioned in the past that your keratosis (or some sort of age spots) hasn’t returned since being on it, so don’t think that you have wasted time and money for nothing.
I wonder if you fingernails have gone back to baby age since you were taking such an enormous amount of Rapa (with GFJ) each time  Now its time for other things to be catching up!!
Now its time for other things to be catching up!!
Anyway, whatever you do, I hope it has a positive effect - you really are a trailblazer for the rest of the community here.
3 Likes
MAC
#44
Love the hacking spirit, but did I miss something on the human translation re meclizine dosing.
“728mg a day for a person at 70 kilo”
How is 25mg/day going to generate a signal?
Although I (n=1) wouldn’t mess with an anticholinergic. Cognitive is my #1 longevity focus.
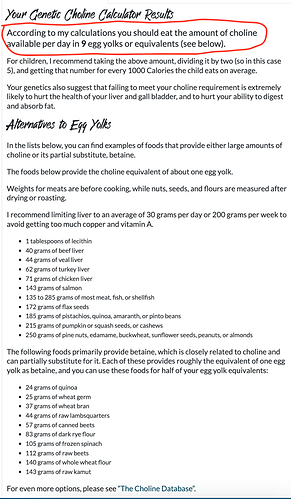
Most people do NOT get enough choline from diet, and depending on your genes, you could be in a HUGE deficit. I am homozygous C677T, so I have been addressing my methylation from start of interventions as a needed bio-hack. You can upload your 23andme into Chris Masterjohn portal, will generate your choline requirements.
My summary shows I should be eating 9 egg yolks/day (1 egg yolk = 164mg choline)…I eat eggs regularly, but have not been consuming 9/day and very unlikely likely getting the daily choline equivalent from the food macros below listing, so I supplement. I eat a lot of nuts and salmon with my keto diet, but even still, likely no getting enough. I don’t eat any liver.
I take 1200mg/day of L-alphagyclerolphosphorylcholine.
Masterjohn isn’t concerned about TMAO, and neither am I based on my research. CM: “On a scale of 0 to 10, my concern for minimizing TMAO is currently a 3. My confidence in this is about 10%, so I consider it highly likely I could change my mind in either direction as new research is published. At the end of the day, choline that your gut microbes turn into TMAO is choline you didn’t absorb, so, at best, it was a waste”
5 Likes
Apparently, my meclizine experiment is going to be short-lived. Stopped taking rapamycin ~two weeks ago and started taking meclizine @25 mg/day. My purpose was to continue mild mTORC1 suppression while waiting to see if my cholesterol levels improved. My levels increased while taking rapamycin at higher dosages of 10 - 20 mg. biweekly with grapefruit juice and olive oil.
I have taken meclizine in the past as a sleep aid and for dizziness and don’t remember any sleepiness problems. 25 mg. of meclizine after my evening meal at ~ 5:30 PM makes me sleep like a baby for ~8 hours. After taking it for a week I find I am sleepy all day. This is probably due to a build-up of meclizine in the blood as its half-life is ~6 hours and doesn’t completely clear before my next dose.
I would like to get my blood markers back to the values before rapamycin. The next time I will have blood work done is in about two weeks. After I get the results I will decide what to do about rapamycin. If my markers improve maybe I will just try cutting back on the rapamycin dosage.
1 Like
RPS
#46
Maybe just take the Meclizine every other day.
MAC
#47
Glad you didn’t go straight for the human translated dose 728mg. You would have woken up next month.
You need to get one of these…that’s how the ITP mice stayed awake at their mega doses. Or in reality, they have a completely different CNS/brain/peripheral metabolism compared to humans.
The ITP is great, but needs context and guardrails…translating to humans is fraught with massive unknowns including likely completely untranslatable genetic/metabolic pathways. And it’s pretty much only a mouse-cancer model. The brains of mice are nothing like human. We are a far more evolved/complex species.

2 Likes
Yeah, I’d ditch the mec and cut back on the rapa.
Maybe meclizine ain’t dead yet:

Agingdoc1MD, PhD
'"However contrast with the favorable: Meclizine ameliorates memory deficits in streptozotocin-induced experimental dementia in mice: role of nuclear pregnane X receptors "
“The upshots of our study proclaim that meclizine protects cognitive deficits by virtue of its antioxidant, anticholinesterase, and antiinflammatory properties.”
2 Likes
As a side note, Dr. Miller at the ITP was enthusiastic about two drugs, Meclizine and Astaxanthin, in the interview referenced above. The problem at the time was that they needed enough mice to die to release a report. The Meclizine report was just released. Here’s hoping the Astaxanthin mice are still alive and kicking for a long time. The longer we have to wait for the report, the more effective Astaxanthin probably is? Has anyone heard an update on this?
P.S. I have been taking Astaxanthin daily with no side effects. Here’s to hope!
5 Likes
Yes - I think the “take home message” from all the meclizine research I’ve seen (and posted above) so far is to be very cautious about adopting Meclizine as an anti-aging drug. The researchers I spoke to at UC Davis said there were many issues with Meclizine given its poor “binding affinity” (and therefore, likelihood of undesirable side effects), but these are academic researchers, not clinicians that have any patience experience so they are talking very generally.
They hope to find other drugs that have both a better binding affinity, and mTORC1 inhibition. Given how long it takes for this type of research to progress, its likely years away before any results towards that goal from this research group, I suspect.
Given the research I’ve seen here, I am in no hurry to add Meclizine to my regimen.
2 Likes
Jay
#53
RapAdmin, Did you ever try Meclizine? If so, what was your experience and what are your current thoughts about using it? For me, as some others have noted, it looks like the effect on BPH symptoms eliminates it from consideration. I’m also not sure about it’s long term mental effects, if any. Could it, like some of the older antihistamines be associated with Alzheimer’s?
I did not. The anti-cholinergic effects seemed concerning to me. I am currently sticking with rapamycin and rapalogues.
JuanDaw
#55
Why wait? If they’re not dead yet, that means it works.
DrM
#56
Thats a lot of meclazine (dramamine), has any one of our self-experimenters tried this? Can you walk afterwards?
I used meclizine for a few months on and off, taking as much as 3x25mg sublingual tablets after supper or at bedtime.
It seems very clean and has a good safety record. It is used by all age groups. I found it to be very effective with no “hangover” or daytime drowsiness effect. From the papers I have looked at it seems less problematic for the elderly than other sleep aids.
Forget the relative risk. The absolute risk is very small, IMO, for even the elderly “Relative risk can be misleading as it does not provide information on the overall likelihood of the side effect happening.”
1 Like
I was initially enthusiastic about these study results since it “seemed” to have fewer side effect issues than rapamycin, but when I learned about the link to dementia I became much less enthusiastic.
Meclizine has a score of 3, on the cognitive burden scale as shown above… this doesn’t seem to be a good thing. I’ll take the occasional canker sore and rash that I get with rapamycin over increased dementia risk.
2 Likes