I am starting to favor a mix a dulaglutide and tirzepatide or retatrutide to get the full mix of crossing the BBB and having potent activation of peripheral GLP-1/GIP etc.
Have you had your ApoE tested? I have one ApoE4, this is why I’m being a little more aggressive at prevention at this point.
People typically get away with things like dulaglutide without huge weight loss. If you have a tendency to be a bit fat, a mix is good, if you risk sarcopenia, then dulaglutide monotherapy would be my pick.
Sadly the Tadalafil seems great for cardiovascular risk, but recent data has had me stop promoting it for neurocognitive decline. There definitely is a strong correlation between taking these drugs and having lower neurocognitive risk - but seems like this is all confounded, which is annoying. Still good for the vascular system.
6 Likes
Which would argue for adding a SGLT2i to the GLP-RA, so as to lower BG and thus potentiate less of the insulin release, as less insulin sloshing around in the system seems advisable vs cancer and generally aging… maybe?
3 Likes
Davin8r
#418
Hopefully! That’s what I’m doing 
2 Likes
adssx
#419
I meant the winner among commercially available single GLP-1RAs (so excluding tirzepatide and products in the pipeline). Hopefully we’ll see more papers like that using more recent data and looking at different countries to find the best product.
Intuitively, I thought dulaglutide would be best based on its BBB crossing. But we now have two association studies pointing to semaglutide. Also: Novo Nordisk is spending millions for a large phase 3 trial of semaglutide on Alzheimer’s while Eli Lilly is doing nothing for dulaglutide. Surely they know best the potential of their drugs. Follow the money…
4 Likes
adssx
#420
Muscle Mass and Glucagon-Like Peptide-1 Receptor Agonists: Adaptive or Maladaptive Response to Weight Loss? 2024
This primer aims to address whether muscle-related changes associated with weight loss treatments such as GLP-1 RAs may be maladaptive (ie, adversely affecting muscle health or function), adaptive (ie, a physiologic response to weight loss maintaining or minimally affecting muscle health or function), or perhaps an enhanced response to weight loss (ie, improved muscle health or function after treatment). Based on contemporary evidence with the addition of studies using magnetic resonance imaging, skeletal muscle changes with GLP-1 RA treatments appear to be adaptive: changes in muscle volume z-score indicate a change in muscle volume that is commensurate with what is expected given aging, disease status, and weight loss achieved, and the improvement in insulin sensitivity and muscle fat infiltration likely contributes to an adaptive process with improved muscle quality, lowering the probability for loss in strength and function. Nevertheless, factors such as older age and prefrailty may influence the selection of appropriate candidates for these therapies because of risk for sarcopenia.
1 Like
Sema is not the best in class for weight loss with respect to GLP1-R’s
Tirzepatide (Tz) is great for weight loss and appetite suppression. BUT Retatrutide (Rt) it is better at weight loss with less appetite suppression. How is that possible? Even if you eat a bit more, Rt will still enable better weight loss. Here is a breakdown on 3 of the common GLP1-R drugs and how they work with regard to appetite and weight loss.
- Ozempic/Wegovy = Semaglutide - GLP1-R only, excellent appetite suppression and just OK weight loss.
- Mounjaro/Zepbound = Tirzepatide - GLP1-R + GIP, excellent appetite suppression and good weight loss - better than Sema
- Retatrutide - GLP1-R + GIP + GCGR, moderate appetite suppression, excellent weight loss - better than TZ
Each GLP1 drug will enable weight loss through 1) appetite reduction, 2) glucose management, 2) slowing digestion to increase fullness. Those 3 functions are a form of caloric restriction, eat less, use it more effectively and lose weight.
Adding GIP helps Tirzepatide with weight loss by increasing the feeling of “fullness” or satiety. This further enhances a reduction in caloric intake, eat less, lose more.
With Retatrutide it has the benefits of GLP1-R + GIP + GCGR. GCGR stimulates the most important type of fat in our body, brown fat and initiates thermogenesis, i.e. burning fat.
We have 3 basic fat types, 1) white (adipose), 2) beige (white in the process of turning brown) and 3) brown fat. Brown fat is what we want more of as it is thermogenic, it metabolizes (or burns) white fat. GCGR also helps white fat transition to beige and then on to brown. While the first 2 drugs in the above list work primarily by caloric restriction, Retatrutide is the only one that actually increases fat burning regardless of caloric input.
This means that with Rt you can theoretically eat more and still lose weight effectively. 1 shot a week, could not be easier.
5 Likes
Interesting insight into the social media “muscle loss” hype with GLP1-R’s. I’ve posted my opinion on this previous to seeing this information.
My opinion was based on being a butcher when I was a kid  and a lover of steak as an adult.
and a lover of steak as an adult.
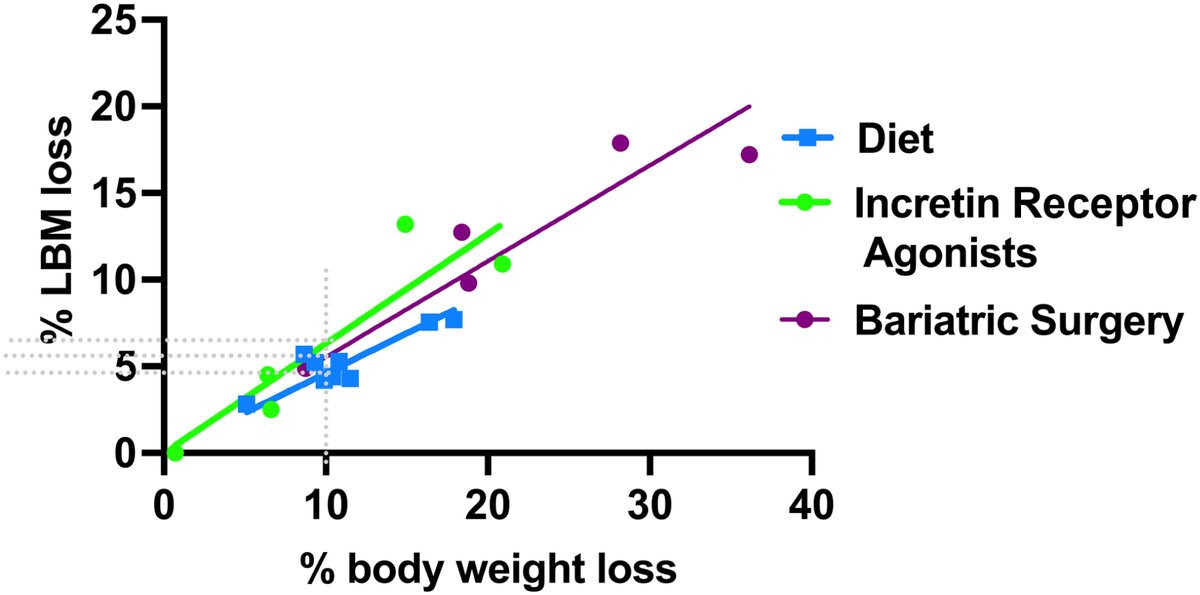
I’ve used the steak analogy a few times. Take a look at Wagyu steak and it’s all about the marbling, i.e. inter-muscular fat. This fat affects the size of the “muscle”, it fluffs it up. Now put that cow on a diet and the muscle will absolutely shrink due to the fat loss. I think a lot of people jumped on the muscle size reduction as an complete indicator of muscle loss when it’s not all muscle fiber loss, a lot of the “size” is inter-muscular fat loss.
Yes some muscle fibre may be lost in any weight loss program but it is relatively easy to counter that with weigh bearing exercise and adequate intake of quality protein.
I was previously corrected by another member on the performance of my Withings Body Cardio scale, which indicates a way higher amount of muscle than it should. BUT, while that data may not be correct as far as an absolute number of my muscle weight, it does show a trend over time. For me that trend is basically flat. FWIW - As a percentage my muscle has gone up as my fat content has gone down.
Intermuscular adipose tissue (IMAT) is fat that is located between and around skeletal muscle groups, and is also known as skeletal muscle fat or lipids. It is considered an ectopic fat depot, similar to visceral adipose tissue (VAT) in the abdomen.
3 Likes
adssx
#423
Oral version of Novo diabetes drug protects heart health in large study 2024
The medicine, which Novo sells as Rybelsus, cut the risk of cardiovascular complications by 14% when added to standard therapies in people with diabetes and heart disease.
Novo intends to ask the Food and Drug Administration around the end of 2024 to approve the medication to protect the heart health of people with diabetes. Should the FDA agree, Novo’s pill would join diabetes medicines like Boehringer Ingelheim and Eli Lilly’s Jardiance and AstraZeneca’s Farxiga, which are proven to have similar benefits.
Novo said that roughly half of study volunteers got a so-called SGLT2 inhibitor like Jardiance or Farxiga during the trial and likely benefited from taking them. Nonetheless, Rybelsus was associated with a reduction in the risk of infarctions, strokes and death, though Novo didn’t disclose more specifics beyond the 14% figure in Monday’s announcement.
SOUL: Oral Semaglutide Cuts CV Events in Diabetic Patients 2024
The majority of patients enrolled in SOUL were taking metformin and about 70% had CAD, 42% had CKD, 21% had cerebrovascular disease, and 15.7% had symptomatic PAD. Additionally, nearly one-quarter had heart failure and 49% were taking an sodium-glucose cotransporter 2 (SGLT2) inhibitor at some point during the trial.
On the basis of these results, which are expected to be presented at a scientific conference in 2025, Novo Nordisk said it plans to file for a label expansion for Rybelsus with both the US Food and Drug Administration and the European Medicines Agency by early next year.
Really good news. Can’t wait for the detailed results to see the effect of the SGLT2i + Rybelsus combination. And also stratification by BMI.
3 Likes
I know I keep boring in on this point, but this is in people with morbidities, diabetes CVD or both. It stands to reason that medications designed to help with disease - help with disease, altough it’s fantastic that they cross help synergistically. What this does for those without these morbidities would be the really interesting news. Specific n=1 respose matters most to individuals, regardless of general statistical cohort response. But I am very happy for those these drugs help.
3 Likes
adssx
#425
You’re wrong. Semaglutide was designed for diabetes, not for overall cardiovascular health. So far only SGLT2i had cardiovascular benefits beyond pure glycemic control. So this is big news. So for people with diabetes or prediabetes, rybelsus might be the best option (compared to, for instance, metformin).
Of course, we need more data on semaglutide on people without these morbidities.
(Btw, I’m not diabetic, I started oral semaglutide a few weeks ago; I’ll report my results; so far, I have lost a few kg (and fat % has slightly decreased), and my HOMA-IR has decreased for the first time (from 1.4 to 1.1, previously SGLT2i had no effect on my HOMA-IR). TBC…)
10 Likes
RapMet
#426
Would you mind sharing the dosage, and if possible, the source of your oral semaglitude. Have gotten a quote from one person, but I like to stick with product that other people have already tried (and it worked for them) before. There is always the fear of getting fake/non-working meds from oversees. thanks
1 Like
adssx
#427
The regular official one. Started with 3 mg. Now at 7 mg.
2 Likes
RapMet: I ordered Rybelsus semaglutide from Jagdish Nikose at RLPharma in India. The meds were packed as “strips”, each strip containing ten pills, each pill individually packed in a blister. I ordered both 3 and 7 mg. The box containing the strips has the Novo Nordisk label. Am planning to re-order.
4 Likes
Let us know whether 3 mg or 7 mg is preferable after your experiment!
adssx
#430
3 mg is the starting dose, described as “non therapeutic”, to get used to the drug. So I’m not using it.
1 Like
How much is Jagdish selling the 7 mg pills for?
For Rybelsus Jagdish quoted $55 for ten pills, 7 mg and $45 for ten pills 3 mg.
2 Likes
cl-user
#433
FYI. Just ordered that from Maulik (maulik7@gmail.com)
Rybelsus Semaglutide Tablets 14 mg x 30 - 129$
5 Likes
Davin8r
#434
I hope you guys tolerate Rybelsus better than I did. I was so sleepy/exhausted I could barely keep my eyes open, and even then the appetite suppression wasn’t dramatic. Subcutaneous tirzepatide, even at very low doses, worked SO much better (although increased HR and fatigue were still an issue to some extent).
That being said, there is a huge amount of variability in both responses and side effects with the GLP meds from person to person, so you may do just fine.
@cl-user you only ordered the 14mg tablets? I hope you aren’t planning on starting at that dose if you’re new to GLP meds because you could end up in the hospital. Splitting the tablets may or may not work since they have a special delivery system through the stomach wall.
3 Likes