adssx
#6
OK, thanks. I’m afraid it’s too good to be true as most studies found no impact of ezetimibe on dementia according to the 2023 Scientific Statement From the American Heart Association on Aggressive LDL-C Lowering and the Brain:
Ezetimibe blocks the absorption of cholesterol from the small intestine and affects expression of adipogenic genes such as peroxisome proliferator–activated receptor-γ, which is decreased with ezetimibe treatment.However, little evidence is available on its effects within the brain or crossing the BBB. […] Randomized placebo-controlled studies of ezetimibe and PCSK9 inhibitor have also failed to find an association between these LDL-lowering therapies and dementia or impaired cognition, regardless of the LDL-C achieved (Table 4). […] Furthermore, a systematic review of 22 randomized trials in 117 781 patients treated with statin, ezetimibe, or PCSK9 inhibitors concluded that these treatments were not associated with cognitive impairment and that a low LDL-C level did not affect the incidence of cognitive disorders or global cognitive performance.
8 Likes
I have not scrutinized the paper yet, but my understanding from the abstract is that the impact is through disrupting a particular protein aggregation pathway—totally unrelated to LDL-C / ApoB etc. Also, this was in vitro only, so there’s no clinical data here. You have to think about what type of clinical study would show benefit based on this causal link. I am not certain, but it reads to me as potentially modifying the long, invisible buildup of protein aggregates that precedes symptoms. So I would think you’d need to take a bunch of APOE-e4/e4 subjects between like 45 and 65 and treat half of them with ezetimibe and track incipient symptoms. I don’t know how much you could compress the timeline. Alternatively, you could do an observational study and just try to find reasonable matched-pairs with and without Ezetimibe prescriptions and compare dementia rates. I don’t know that we would expect it to be a cure or treatment for existing AD based on the hypothesized mechanism of action.
3 Likes
adssx
#8
It’s true that even though ezetimibe is a common drug, observational studies and emulated trials about lipid-lowering therapies and dementia (there are many of them) often only look at statins or group all “non-statin therapies” (including fibrates) in one bucket. So it would be nice to have one study specifically on ezetimibe and AD and all-cause dementia. Hopefully this paper will trigger research in this area.
6 Likes
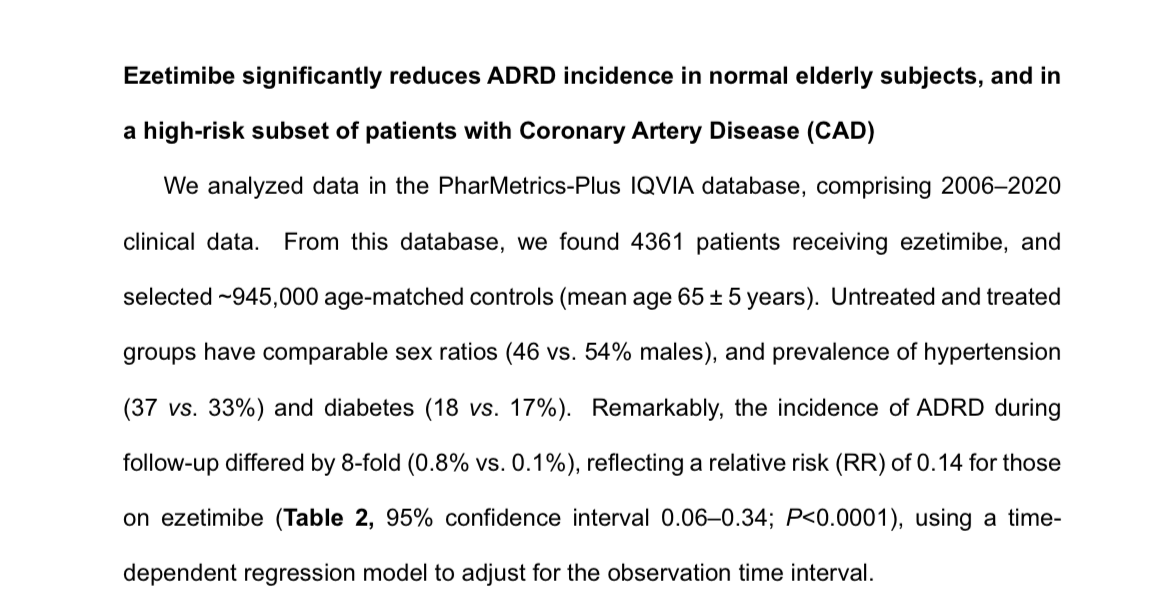
I read through the paper, and they actually did present observational results. That’s where that 0.14 hazard ratio came from. So they’re claiming a potential ~eight-fold reduction in risk observed in patients taking Ezetimibe (obviously for other indications).
5 Likes
adssx
#10
Thanks a lot. It’s quite impressive, but they only controlled for age?! Not for LDL? People using ezetimibe usually also use statins, so most people on ezetimibe probably have lower LDL than non-treated individuals. It would be better to compare cohorts of ezetimibe users (monotherapy?) to other lipid-lowering therapies
4 Likes
adssx
#11
Actually they did something similar and found an even better RR:
A subset of these subjects had been diagnosed with Coronary Artery Disease (CAD). Among those with CAD, we identified 547 patients prescribed ezetimibe and 73,387 CAD/CHD age-matched controls. In this cohort, with a known elevated likelihood of subsequent AD or related cognitive impairment, the relative risk for ADRD diagnosis during follow-up was 0.122 for ezetimibe recipients relative to controls (Table 3, 95% C.I.: 0.02‒0.88; P<0.006).
6 Likes
Usually, Ezetemibe is prescribed as a follow-up drug meaning that individuals that are taking it are usually taking a statin, BP medicine, T2D meds, and others. There could be a lot of other confounding medications/factors.
What the study does tell me is that Ezetemibe is a useful drug to add to the mix of whatever drugs are usually prescribed beforehand.
2 Likes
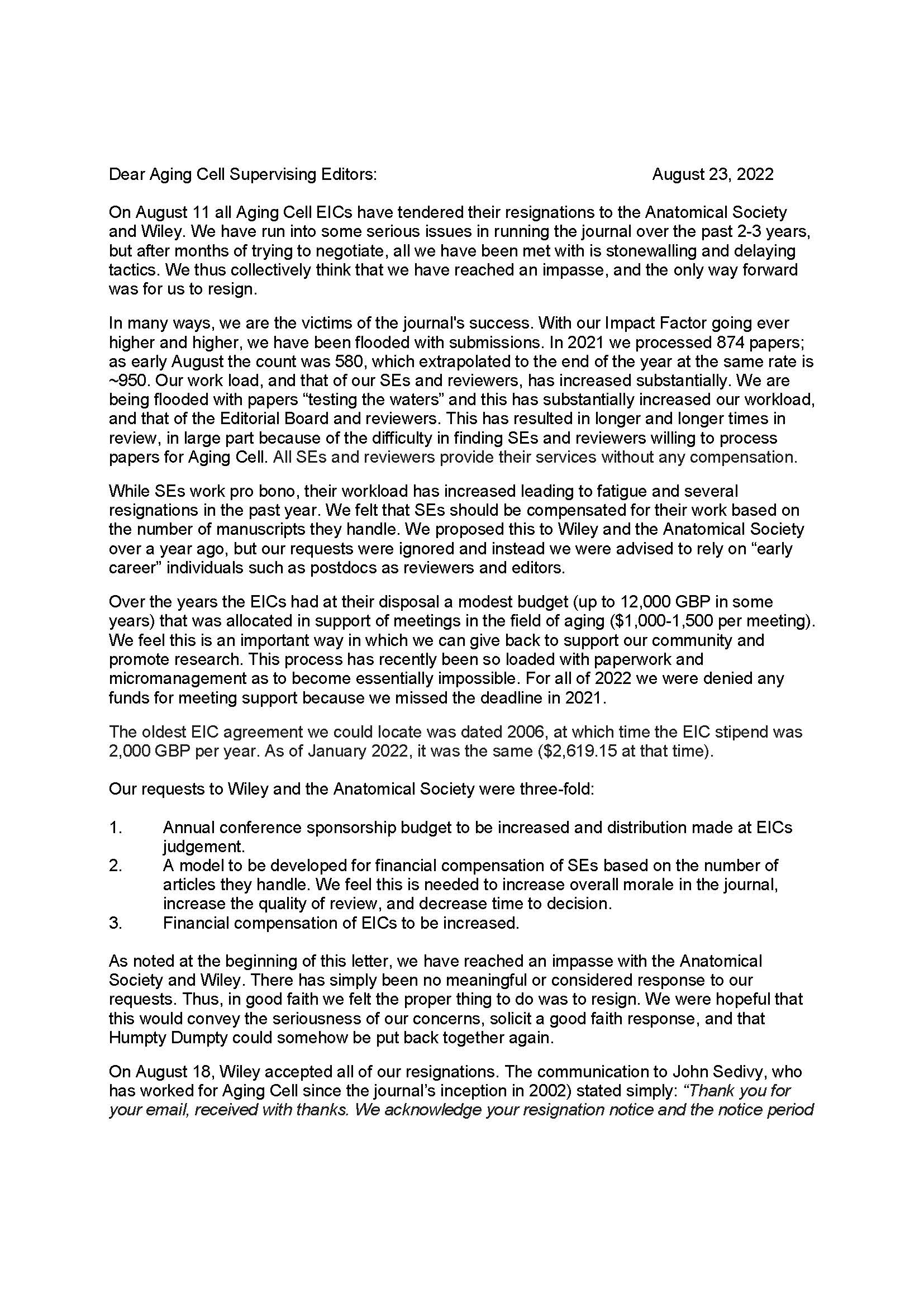
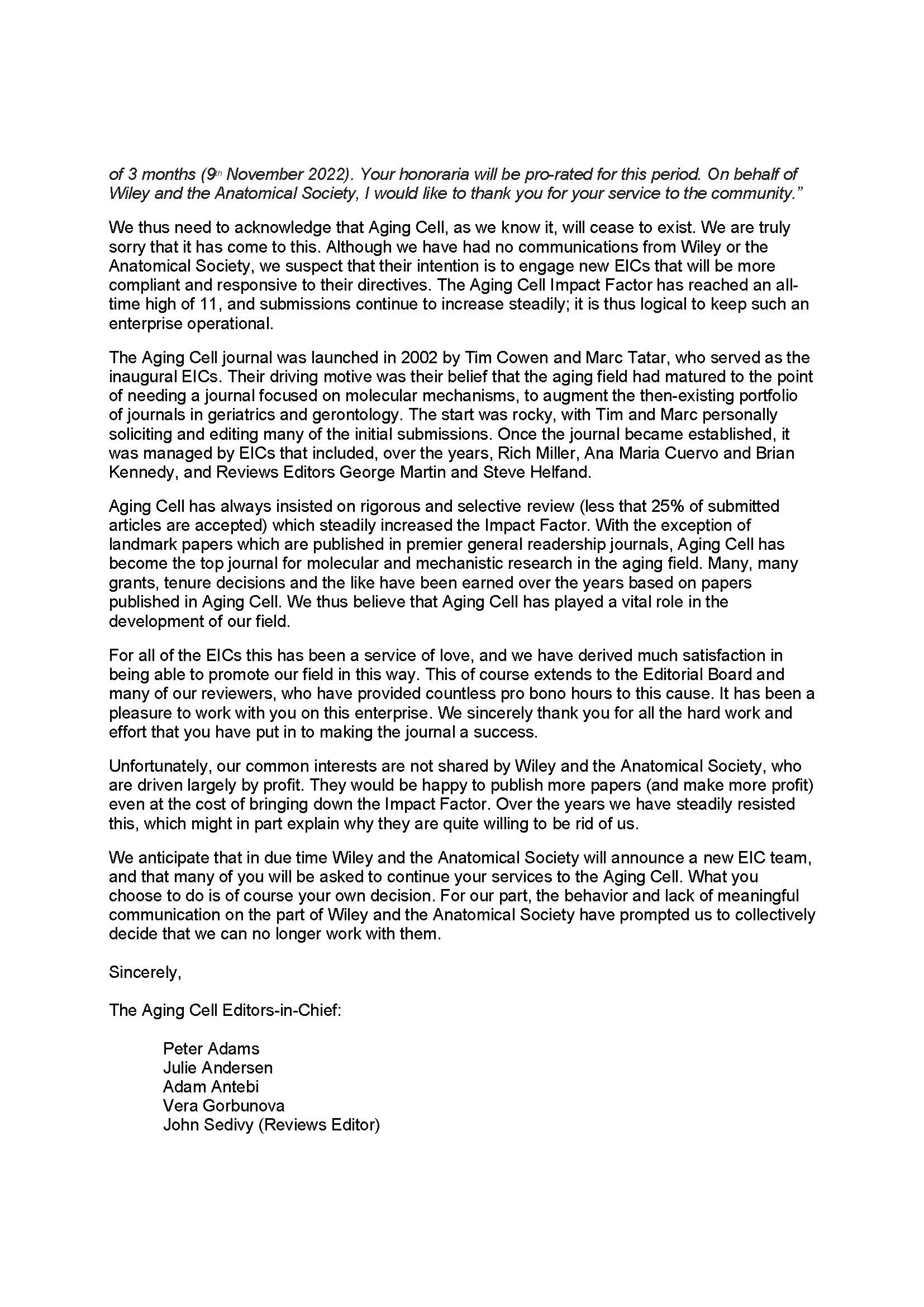
The paper seems to be an upstart/spinout of another well-known journal… I forget what exactly the disagreement was around though:
Aging Biology was founded by former Editors in Chief of Aging Cell.
In 2022, a dispute with the publisher resulted in the resignation of five editors in chief and majority of the editorial board that went on to establish Aging Biology. We will continue the tradition of publishing high quality science with the review process run by the leading scientists in the field of aging.
more…, it seems to be a legitimate journal. The Editors in chief are all well-known researchers. The reason for the new journal seems reasonable.
3 Likes
I had a bad reaction to this drug. Severe sadness to the point of despair. And that is a reported side effect. Also brain fog. I couldn’t figure out what was going on because nothing in my life had really changed. Then I looked up the side effects and “sadness” was one of them. I had never seen that as a side effect for a pharmaceutical. I was often on the verge of tears for no apparent reason. As soon as I stopped the drug my normal generally good mood came back. Weird.
8 Likes
I hear you. Sometimes a drug will just cause a strange side effect. I’ve had a similar response to Finasteride. Rosuvastatin caused all my muscles to weaken. If a drug doesn’t work for you, don’t force it. Just cross it off the list and move on to the next best thing.
For me, I changed from Rosuvastatin to Bempedoic Acid. For Finasteride, I changed to bald(ing). 
5 Likes
adssx
#16
Are We Using Ezetimibe As Much As We Should? 2024
Lipid-lowering therapies, particularly non-statin regimens, are underutilized as ~2/3 of patients with atherosclerotic cardiovascular (CV) disease (CVD) are not optimally managed, and do not attain target low-density lipoprotein cholesterol (LDL-C) concentrations, despite statin treatment. Statins have been the mainstay of hypolipidemic therapies; however, they are plagued by adverse effects, which have partly hindered their more widespread use. Ezetimibe is often the first added mode of treatment to attain LDL-C goals as it is efficacious and also allows the use of a smaller dose of statin, while the need for more expensive therapies is obviated. We herein provide a comprehensive review of the effects of ezetimibe in lipid lowering and reducing CV events and improving outcomes. Of the hypolipidemic therapies, oral ezetimibe, in contrast to newer agents, is the most convenient and/or affordable regimen to be utilized as mono- or combined therapy supported by data from CV outcomes studies attesting to its efficacy in reducing CVD risk and events. When combined with a statin, the statin dose could be lower, thus curtailing side-effects, while the hypolipidemic effect is enhanced (by ~20%) as the percentage of patients with target level LDL-C (<70 mg/dL) is higher with combined treatment versus a high-intensity statin. Ezetimibe could also serve as an alternative treatment in cases of statin intolerance. In conclusion, ezetimibe has an excellent safety/tolerability profile; it is the first added treatment to a statin that can attain LDL-C targets.
6 Likes
A_User
#17
If people want to live a long healthy life with a reduced risk for stroke and heart attacks they should consider trying ezetimibe.
Whether it might reduce ALA absorption, that can be tested with a Omega-3 ALA test.
2 Likes
Thanks for sharing this. I am on Ezitimibe (5 mg) and have been experiencing sadness as well. Had thought of it as what Freud called “ordinary unhappiness,” the normal response to aging and loss. But may-be it is the drug!
When I stopped, the sadness disappeared within a day or two.
4 Likes
A_User
#20
I had a similar side effect from choline supplementation and apparently it is common for that.
A study I posted earlier (possibly on another thread?) showed that taking ezetimibe at least 4 hours apart from vitamin E prevented the inhibition of vit E absorption, so it would make sense that the same would be true of ALA. I now take my ezetimibe at night, since I put ground flax seed and walnuts in my morning smoothie (both rich in ALA). Also another study showed no inhibition of EPA or DHA, so if you take fish or krill oil, it shouldn’t be a problem.
6 Likes
adssx
#22
3 Likes
adssx
#23
Also an Egyptian paper so might not be of high quality, and it’s an animal model but: Ezetimibe protects against Gentamycin-induced ototoxicity in rats by antioxidants, anti-inflammatory mechanisms, and BDNF upregulation
We know that hearing loss is a modifiable risk factor for Alzheimer’s disease. This paper suggests ezetimibe might be protective:
The threat of hearing loss has become a universal reality. Gentamycin (GM) can lead to ototoxicity and may result in permanent hearing loss. This study aimed to elucidate whether the hypolipidemic drug Ezetimibe (EZE) has a possible underlying mechanism for protecting rats from GM-induced ototoxicity.
EZE can safeguard inner ear tissues from GM via antioxidant, anti-inflammatory, and antiapoptotic mechanisms, as well as upregulation of BDNF mechanisms.
2 Likes
adssx
#24
Editorial from last month commenting on this paper: Hiding in Plain Sight: FDA-Approved Cholesterol Drug Ezetimibe as a Treatment for Alzheimer’s
The authors note that, while the controls (nearly 1 million subjects not taking ezetimibe) were well matched to ezetimibe recipients for age, gender, and established ADRD risk factors such as hypertension, diabetes, and kidney disease, the groups were not matched for cholesterol levels. It would not be unreasonable to assume that the patients prescribed ezetimibe had initiated it due to relatively high serum cholesterol levels, so these researchers point out that double-blind randomized trials of newly enrolled patients would have to be conducted to establish a causal connection.
7 Likes
59vw
#25
Perhaps we shouldn’t be splitting our 10mg tablets to 2.5 mg…
5 Likes