John - have you tracked your CRP over the years as you implemented your protocol? What factors do you think are the major contributors to your low CRP?
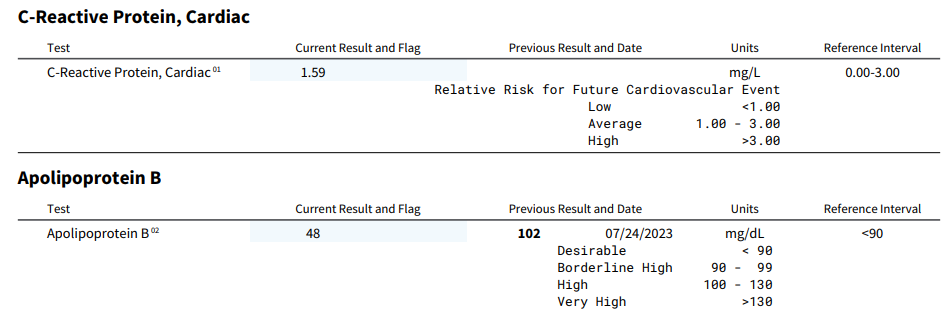
My CRP is at 0.90, and while not bad, I would like to get it much lower.
How to lower high CRP levels: Focus on your risk factors
Since hs-CRP levels reflect the level of inflammation in the body, most ways to lower high CRP levels are focused on reducing underlying causes of inflammation. Making lifestyle changes to reduce inflammation is in your control, but other contributing factors (like autoimmune diseases) may need medical intervention. Due to their effect on inflammatory pathways, some medications may cause a reduction in CRP, such as:
- Statins (commonly used for high cholesterol)
- Non-steroidal anti-inflammatory drugs (NSAIDs) (e.g., ibuprofen and aspirin)
- Corticosteroids (typically used to treat rheumatologic conditions like arthritis)
- Metformin (commonly used to treat type 2 diabetes)
- Vitamin or herbal supplements (e.g., fish oil, anti-inflammatory spices like turmeric and ginger)
There are also several ways that may help reduce high CRP levels naturally:
Eat anti-inflammatory foods
Certain foods are linked to higher levels of inflammation. Limiting or avoiding inflammatory foods like refined carbohydrates, fried foods, red meat and processed meat can help reduce CRP. Instead, focus on eating more anti-inflammatory foods like leafy greens, nuts, fatty fish and whole grains. Over time, an anti-inflammatory diet full of fruits, vegetables and fiber can help lower CRP levels.
Exercise regularly
In the short term, intense exercise like weightlifting or a long run might spike CRP levels. (That’s why it’s important not to exercise immediately before testing your CRP levels.) But in the long term, regular physical activity can have anti-inflammatory effects on the body. Exercise not only helps reduce body fat (which contributes to inflammation), but it can also help the body increase its production of hormones that fight inflammation.
Aim for 30 minutes of moderate exercise at least five days per week. This could include brisk walking, swimming, cycling or other cardio exercises that get your heart rate up. Strength training with weights two to three times a week also has anti-inflammatory health benefits.
Manage your weight
When your body is carrying excess weight, the surplus of macronutrients in the adipose tissues (i.e., body fat) can contribute to inflammatory effects in the body, causing the liver to produce more CRP. In other words, the more fat your body is carrying, the higher your risk of chronic inflammation and high CRP levels.
Losing even a modest amount of weight can help lower inflammation and CRP. Focus on diet and exercise for safe, sustainable weight loss.
Avoid or quit smoking
Smoking triggers inflammation and damages blood vessels, raising your risk of several serious health conditions, including cancer, lung disease and heart disease, among others.
Giving up smoking can help lower CRP levels and inflammation. However, research shows that CRP levels may remain high long-term for those who quit smoking compared to those who have never smoked cigarettes.
Limit alcohol
Drinking heavily promotes inflammation. Moderate your alcohol consumption by limiting yourself to one drink per day for women and two drinks per day for men. Give yourself alcohol-free days each week to allow your body to recover.
Manage stress
Chronic stress takes a toll on the body and can raise inflammation. Make time for relaxing activities like meditation, yoga or deep breathing. Spend time doing hobbies you enjoy. Get enough sleep and connect with family, friends and other people within your support system. Managing stress can help control inflammatory responses.
The key to lowering inflammation is being proactive about your health. Get your CRP levels tested so that you know your baseline and talk to your doctor about your results to make sure you understand them and to see if additional evaluation or intervention is needed.