Good news for those of us stuck with high Lp(a) and no effective treatments.
My last Lp(a) was 84mg/dl. ApoB is less than 40mg/dl now, just for comparison.
2 Likes
Beth
#3
Wow, RobTuck, that is an incredibly long list and a gives us a lot of hope!
A_User
#4
I’m not sure.
10mg Rosu/day, 10mg Ezetimibe/day, 140mg Repatha
Thanks for sharing the study. I check my glucose, insulin, HBA1c and eyesight regularly and they’ve never moved since starting treatment. If they do show any signs of changing, I could look at changing to Atorvastatin.
A_User
#6
You’re waiting for ex-post when you know ex-ante what is expected to happen on average?
Wouldn’t those small changes mean some damage might’ve already occurred?
Just curious about the reasoning.
Glucose, insulin, and HbA1C isn’t that accurate, as far as I’ve heard, OGTT apparently is better.
The only available treatment that can lower Lp(a) by up to 30% are PCSK9 inhibitors like Repatha.
It’s a good question, and it’s nice to challenge our own decision making. But with that said, I think “expected to happen on average” is a bit of a strong statement. In the link it says “The rosuvastatin group had a higher incidence of new onset diabetes mellitus requiring initiation of antidiabetics (7.2% v 5.3%; hazard ratio 1.39, 95% confidence interval 1.03 to 1.87; P=0.03)”.
So, in context, that’s a pretty small chance of new onset diabetes to begin with. I also expect that some % of people in that age bracket would have new onset diabetes just from aging. Additionally, the difference between the groups is small, with a wide confidence internal, and barely scraped statistical significance.
From my POV:
- I am taking a low dose (10mg per day), which is lower than the average in the trial
- Rosuvastatin works, for me, very well at doing the most important thing, which is lowering ApoB
- I seem to tolerate it perfectly well - no elevation in liver enzymes, no muscle pain etc. We know that some people have different tolerance for different statins
- I think my personal risk of having any glucose disposal problem is very low. I have decent muscle mass. I’m reasonably lean. I exercise. There’s no family history of insulin resistance in my family, and my track record of glucose, insulin, OGTTs etc is really strong.
- Changing medications is a bit of a fuss. Asking for a different prescription is easy enough, but then it also means monitoring for effectiveness and any adverse effects, and trying to figure out whether any changes are due to the different medication, or something else.
That said, since this is a lifelong medication and I am still young (less than 40), I will keep open minded that it is something I may change in the future. I’m sure that every year that goes by will bring better evidence and the decisions will become easier.
And I’m already taking Repatha, haha
2 Likes
A_User
#9
By average I mean the median result, and by expected is expected value so you’re expected to increase your risk by some causal mechanism as you’re rolling the dice, one drug over the other costs a few micromorts if all else is equal, i.e it’s worse ex-ante if equal in under treatment side effects.
RobTuck
#10
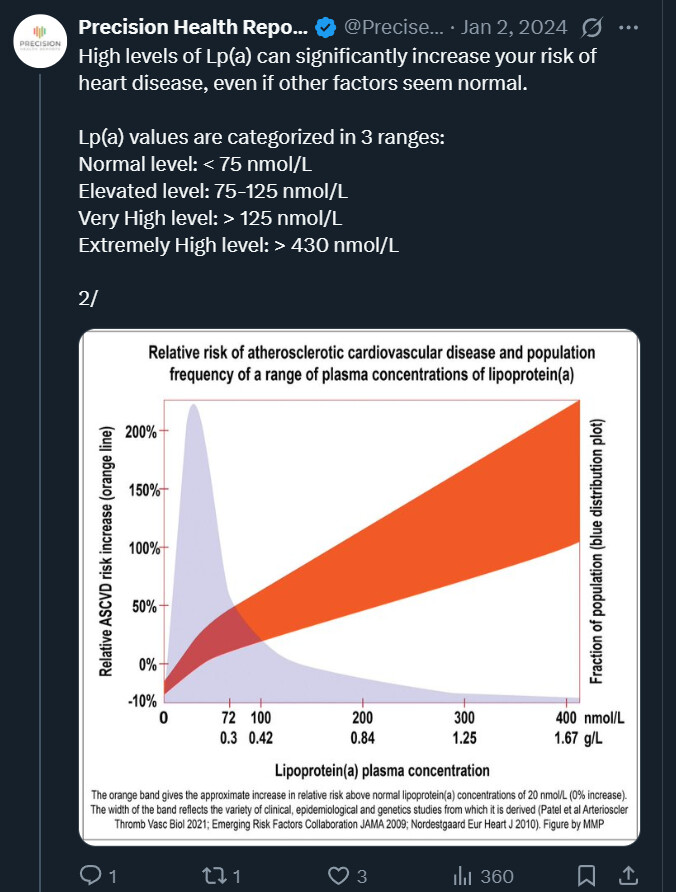
Has anyone seen any data describing, say by quartile, the ASCVD risk curve for Lp(a) according to its level. As new therapies for lowering Lp(a) come to market, the question arises about the level at which it is worth attempting to lower it. I’m reasonably certain that a real curve would be multifactorial, involving among other things Apo(b) but here I was thinking more simplistically.
RobTuck
#12
Thanks. Based on this, an ideal target might be ~20 nmo/L. At 40 nmol/L, I’m close enough to the line that it might not be a priority. What I especially like about this chart (assuming it was done well) is that it implies the mean molecular weight used to convert to/from g/L. Some of my friends have had test results in g/L and the best I could do was give them a range.