LukeMV
#576
Empagliflozin has lowered my uric acid pretty significantly. I’m almost worried it’s too low now at 3.8 as the combo with Telmisartan also lowers it.
4 Likes
DrWill
#578
High and low HDL increase your risk of ascvd.
LaraPo
#579
My June HDL is 96, LDL 78, total 184. Not bad. What do you think?
2 Likes
Bicep
#580
Looks close to optimal to me, possibly the HDL is too high? Maybe your body needs it that way at this time. Good Job.
1 Like
LaraPo
#581
It’s going down pretty fast, together with other lipids and ApoB. Could it be a-cyclodextrin? Are you still taking it? Do you see any results?
Bicep
#582
Yes, it could be. I’ve only tested once since starting, but I’m pretty sure it had a big effect. I’ve quit most everything else.
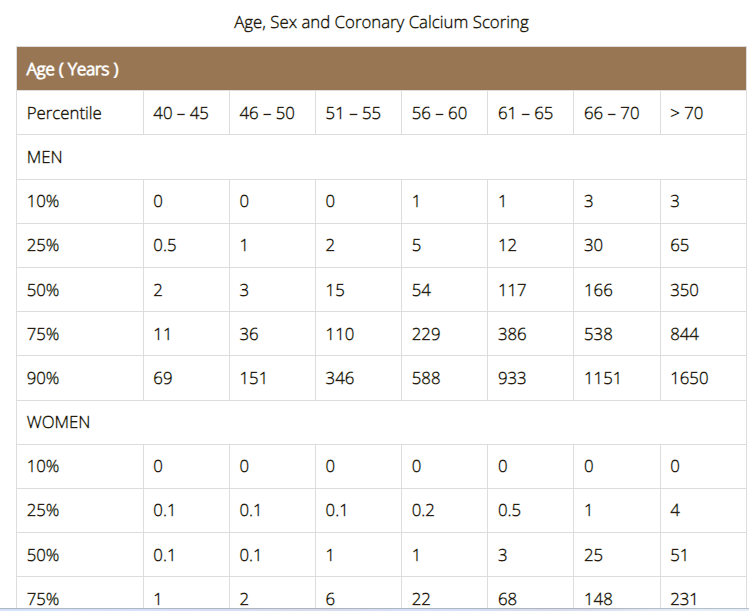
I found this table interesting. Women, in general, have a much lower CAC than men of the same age. I want to be in that lucky top 10%!
https://cardiology.com.sg/coronary-artery-calcium-imaging-scoring/
3 Likes
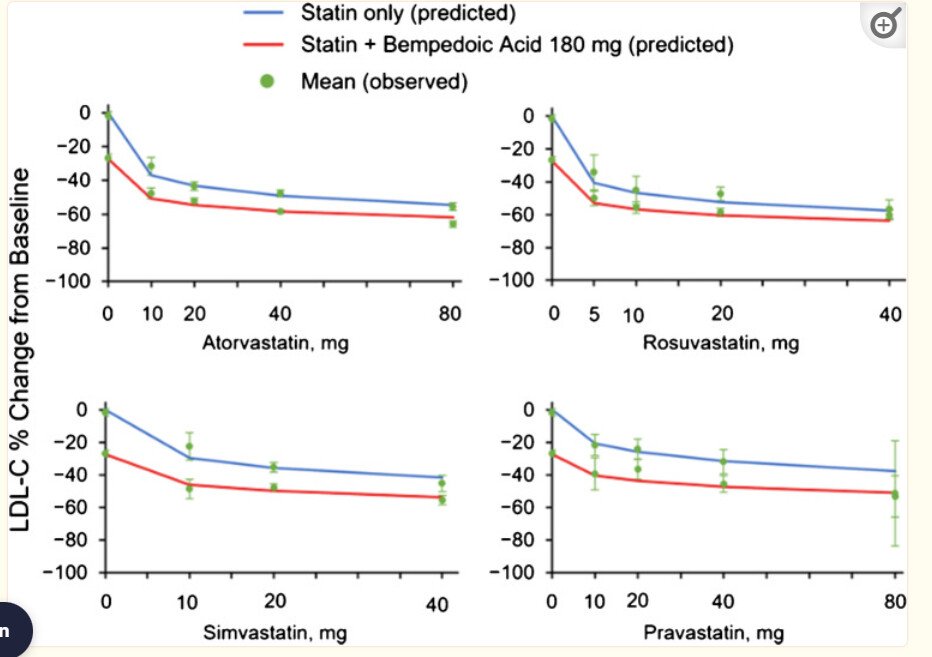
Not sure if this has been posted before. This is the chart that shows combination of statins with Bempedoic Acid in terms of reducing LDL.
It seems that my father can reduce his LDL from 65 to 45 by adding a low dose statin like 5 mg Rosuvastatin or 10 mg Atorvastatin. However, he needs to be careful about GFJ and statins.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9474414/
2 Likes
A_User
#585
Rosuvastatin is not affected by GFJ.
3 Likes
adssx
#586
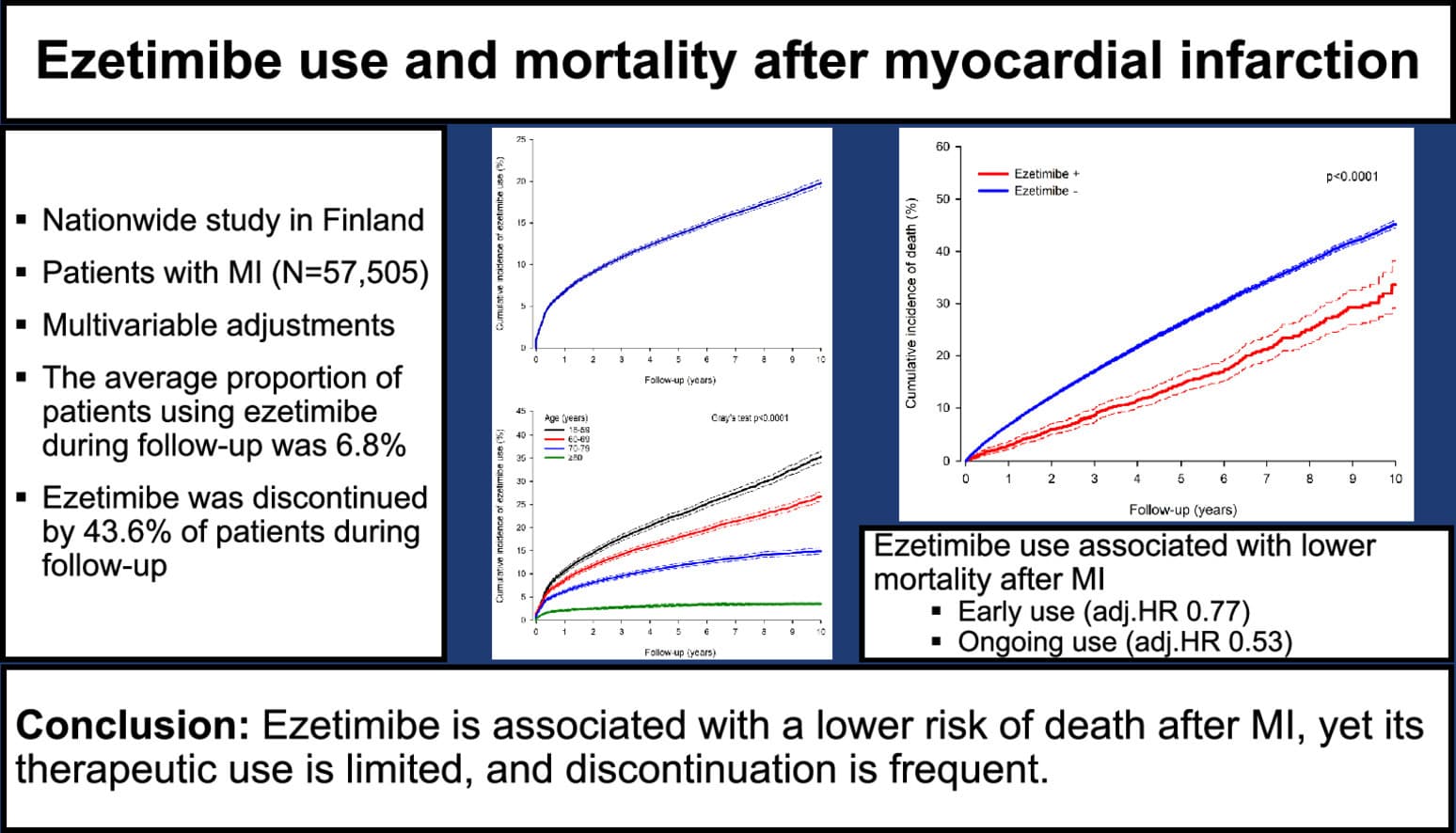
Ezetimibe use and mortality after myocardial infarction: A nationwide cohort study 2024
Comparison of Moderate Intensity Atorvastatin and Ezetimibe with High Intensity Atorvastatin on Cardiovascular Events and Diabetes in Patients with Angina Pectoris Undergoing Percutaneous Coronary Intervention 2024
During a mean follow up of 4 years, there were no significant differences in the cardiovascular outcomes between high-intensity atorvastatin monotherapy and moderate-intensity atorvastatin and ezetimibe combination therapy. The adjusted hazard ratio (aHR) for cardiovascular death was 1.18 [95% confidence interval (CI): 0.87-1.61, p=0.285], MI was 0.82 (95% CI 0.67-1.01; p = 0.066). and stroke was 1.10 (95% CI: 0.86-1.39, p=0.453), respectively. The risk of new onset diabetes was not different between the two-treatment group (aHR: 0.99, 95% CI: 0.88-1.13, p=0.94).
7 Likes
Why is Eze frequently discontinued? I haven’t noticed any side effects from taking it.
Beth
#588
My doc warned me many have unpleasant tummy effects… diarrhea etc.
hitch
#590
Marek Health has apoB test for $17 (plus $5 puncture fee at LabCorp)
4 Likes
I hope this is the best thread to put this on, if not, if someone can transplant it to the best one. I know the issue of variability in Lp(a) testing has been a discussion point.
One of the issues Dr. Dayspring details in this podcast
https://theproof.com/new-heart-disease-test-you-should-order-thomas-dayspring-md/
Is how Lp(a) works in regard to lab testing, and due to varied molecular weight, the mg/dL is probably not the ideal way to measure, but this is the standard in the labs I utilize. The molar concentration (e.g. the number of particles) is the more stable situation.
Anyway, I found this podcast to be informative and a really valuable addition to my understanding in this area. Hopefully other listen and expand their knowledge also.
9 Likes
LabCorp gives Lp(a) results in nmol/L, if you’re able to order labs from them.
2 Likes
A_User
#593
Has this cardiovascular health issue been resolved at this point in the forum, I feel like I don’t see much denialism of LDL or apoB and Lp(a) with cardiovascular disease anymore? They simply lost, the grifter* who wants the facts to fit with their opinions and biases are too exposed with evidence.
*Usually it is someone who wants to eat keto in a specific way, high in saturated fatty acids, and who has to deny any negative consequences of their choices.
1 Like
You are absolutely right - I was pretty sure that the labs were reporting in mg rather than nmol/L
I looked at mine from 2023 from Quest … and the units were nmol/L … so being measured in a way that should be more stable than if not measuring by the molecule per unit of volume.
Anyway, this presentation with Dr. Dayspring was pretty useful in filling in knowledge.
2 Likes
Dr. Brad believes you can get rid of plaque.
5 Likes