A_User
#2395
Now that I think about it technically if that’s the case you could then try different mTOR inhibitors or rapalogs like everolimus, or switch SGLT2 inhibitor.
I think most SGLT2i have a similar lipid impact (which is minimal to begin with), and rapa has a lot more data behind it (wrt. health benefits) compared to any other mTOR inhibitors, so my instinct would be to keep these two (as I suspect they’re not responsible - I’ve always had sh|tty lipids), and instead crush my ApoB with more powerful drugs. 
1 Like
A_User
#2397
We have the Mannick 2014 everolimus study in humans, 2-year carcinogenicity studies showing mortality and observed aging benefit, and some unpublished lifespan data. I’m not sure the data on rapamycin is that much better.
Fair points. However in animal models there’s definitely more data on rapa - possibly one should not be too influenced by animal data, but in general there isn’t much longevity/health data for sirolimus/everolimus in humans anyway, so animal models is what we extrapolate from (with all attendant dangers of such).
A_User
#2399
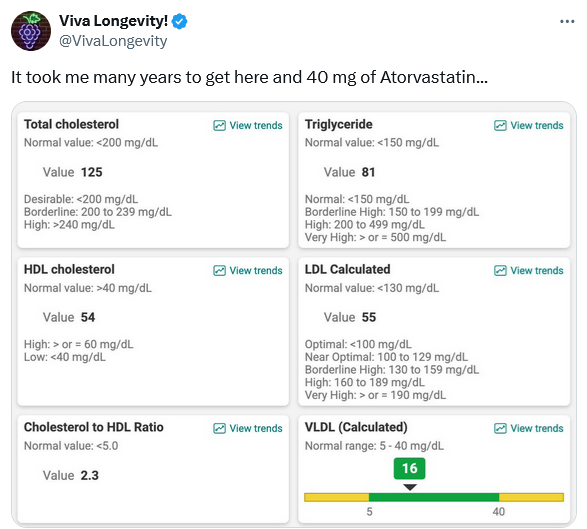
https://x.com/VivaLongevity/status/1956164444683190414#m
Since Viva Longevity is in academic circles, I wouldn’t be surprised if he got advice by a Ivy League doctor, it checks out. High intensity statin. They loveeee it.
1 Like
Well, it took him many years. Looking at my own case, if I can ever get to reasonable lipid numbers, it wouldn’t surprise me if it takes years of experimenting.
Sorry you are having to deal with this! Hoping it gets better! 
2 Likes
Beth
#2402
I’m not worried about you in the least, but just thought I’d share my LDL was 131 in March 2018 and dropped to 55 by October of 2018, from repatha alone.
I only added ez and ba in the past year, and it’s now 41. No statins, so all the heavy lifting was repatha.
4 Likes
adssx
#2403
Thanks for sharing your experiment. Here’s my ezetimibe 10 mg (only) experiment (before => after, in mg/dL):
- Total cholesterol: 199 => 143
- LDL: 128 => 73
- ApoB: 97 => 62
- HDL: 58 (constant)
- ApoA1: 150 (constant)
We’re all different and I guess the only way to know today is to… Give it a try and measure
7 Likes
Beautiful values. A 43% reduction in LDL-C and 36% reduction of apoB with just ezetimibe alone is remarkable.
1 Like
adssx
#2405
Hyperresponder to ezetimibe and therefore probably hyperabsorber of cholesterol.
4 Likes
adssx
#2406
Averages hide a lot of inter individual variations:
Source: Ezetimibe Reduces LDL-C for HIV+ on HAART
Some people see LDL increase with ezetimibe! (although it might be due to other things that changed in their life during the trial over that period)
2 Likes
I think the increase in LDL for those on Ezetemibe is similar to the increase in LDL in the placebo group, but it is still lower overall. The increase in LDL is probably a byproduct of other factors that may raise it.
2 Likes
A_User
#2408
Where are the LDL Cholesterol skeptics?
1 Like
Bicep
#2409
Lol, happily living their lives. Though the heat and humidity here have been nasty and I spent the morning scooping sh-t out of a pit under our grain leg. So maybe not all happy.
1 Like
L_H
#2411
I’m interested in his source for the 30-60 LDL-C figure. It seems a little exaggerated which is consistent with other academics in this area.
LDL-C levels in hunter gatherers and non-human primates aren’t heavily researched. I’ve had another search and still the best data is only estimated from total cholesterol and is in a higher range.
“Evidence from hunter-gatherer populations while they were still following their indigenous lifestyles showed …These populations had total cholesterol levels of 100 to 150 mg/dl
with estimated LDL cholesterol levels of about 50 to 75 mg/dl.”
https://pdf.sciencedirectassets.com/271027/1-s2.0-S0735109700X02707/1-s2.0-S0735109704007168/main.pdf
Worryingly when you Google it - AI now says ‘40 to 60’ quoting the very tweet you pasted!
Is this how human knowledge is AI’d into sludge?
I can see the temptation to exaggerate down, in the face of a global population marching unwittingly towards atherosclerosis, but I do worry that Google Gemini is requoting unsourced tweets!
2 Likes
FWIW, when I use AI to assist in research, I ask for sources in the prompt. I then follow up and check all the sources because I worry about hallucinations. Also, I find (at least so far), that AI (Google Gemini, ChatGPT) is poor in assessing the quality of the evidence it comes across (studies etc.). In general AI has the tendency to answer the questions it has the answers for, rather than the question you ask, and it can actually ignore your explicit prompts even as you ask it to revise the research plan, because it keeps coming back to what it knows, it’s very hard to get it to break out of those loops it gets trapped in like in a bubble - the “reasoning” ain’t reasoning. But I have not used those dedicated medical platforms, so maybe those are better, though I doubt it, as it strikes me as a structural problem. Maybe it’ll improve down the road.
Atherosclerosis did exist in the past as well
https://www.sciencedirect.com/science/article/pii/S1936878X11000660
However, it may be that the life of the egyptian pharaohs was quite different and that caused atherosclerosis.
I think the whole argument is a red herring.
We aren’t hunter gatherers or chimps. We don’t live as they live(d), and it doesn’t matter what their lipoprotein and cholesterol levels are. Human life expectancy is now longer than our ancestors, and in 2025, LDL-C is causitive of the biggest killer. We have tools to lower it, and they have already been shown to help people live longer. There is also no strongly-detectable signal that lowering LDL-C is harmful.
Those are the only things that matter.
Otherwise we’re just playing into silly arguments by people who are arguing in bad faith, trying to stir up controversy. It’s a fallacious argument in the first place that historical or natural ways were better. Buying that argument would have us dying during childbirth, dying of untreated minor infections, dying from childhood asthma, and yes, dying from ASCVD.
3 Likes