So now my idea is to add bempedoic acid + ezetimibe to my low dose of atorvastatin. Would love a PCSK9i, but alas, can’t afford the cost.
1 Like
Pat25
#984
Has anyone been taking solely bempedoic acid + ezetimibe without taking a statin, and kept track of their LDL/trigs/ApoB levels?
Do we know if just this combination without a statin could also yield good results?
A_User
#985
Yes, it lowers LDL by about the same as a moderate intensity statin.
So if someone doesn’t want to take statins for whatever reason this is available, and inexpensive if you live in the U.S. and can order from India.
4 Likes
Pat25
#986
Fantastic, thanks Anuser.
It would be great if we would have a thread or poll what approach members follow with regard to taking statins and/or (a combination with) bempedoic acid + ezetimibe.
Generally I’m wondering from what age and with what LDL/trig/ApoB numbers most members here would consider taking a statin and/or (a combination with) bempedoic acid + ezetimibe.
Is it indeed a better idea to start taking these from a (relatively) younger age, and pushing these numbers further down, even if they are not yet outside the ‘normal’ range?
adssx
#987
We could start a poll “What’s your LDL target?” with options like < 50 mg/dL, < 70, < 100, < 130, “I have no LDL target”.
For Bempedoic Acid and Ezetemibe results, see here:
1 Like
Pat25
#989
That would be great. Perhaps ApoB values could be included also?
And what about age as a factor?
adssx
#990
We can only do polls with one parameter on this platform.
1 Like
Pat25
#991
Well, imo the LDL-poll could be a great start to get an impression of the approach other members follow.
I think the medical consensus is that the more you push ApoB/LDL down and the longer you do so (i.e. start at an earlier age) the better the health outcome. Statins of course are not tolerated by all, and for some there are consequential side effects (like glucose control), but they have the longest track record. PCSK9i dont’t have as long one, but on the other hand they are based on the same mechanism that allows some natural populations with gene variants equivalent in effect to PCSK9i a long atherosclerosis and CVD free life. Bempedoic acid is newish. But back to statins - the other aspect of statins is that while they do have side effects, they also have pleiotropic positive effects on cancer and a slew of health conditions, possibly by lowering inflammation. So if you can tolerate statins you might want to take them regardless of your lipid numbers, as studies seem to show benefits for even normal-lipids folks, and the lower the better.
3 Likes
adssx
#993
Statins are great but, as a reminder, they’re not risk free either: Statins aggravate insulin resistance through reduced blood glucagon-like peptide-1 levels in a microbiota-dependent manner. In people with Parkinson’s they also aggravate motor symptoms.
3 Likes
True enough. However, the net effect seems to still be a positive from a health/lifespan point of view. Same as rapa - side effects, but net positive. And that’s the temptation of polypharmacy - trying to counteract the side effects, some times with success: ITP results tell us combining glucose impact meds with rapa is a further boon. But naturally, polypharmacy drastically increases the risk of unwanted negative interactions.
2 Likes
Many cardiovascular patients will take around 15 prescription drugs in order to stabilize their condition. I think many people are unjustly afraid of polypharmacy.
I’d say it’s best to take some prescription drugs to prevent cardiovascular problems instead of taking more after you have a cardiovascular problem.
2 Likes
mccoy
#996
I’ve been searching and pondering further but in my ideal optimization, which aims to provide the best results at the best risk profile, taking mini doses of ezetimibe+statin, pill geometry is the governing factor.
I could only find circular-section pills in Rosumibe 5/10 (10/10 is oval) and Crestor 5 mg.
So the strategy I previously hinted at remains so far the only possible, barring further research.
-Day one: 1/4 pill of rosumibe 5/10; Provides Ezetimibe= 2.5 mg, Rosuvastatin 1.25 mg
-Day two: 1/4 pill of Rosuvastatin, provides 1.25 mg
-Day three: 1/4 pill of rosumibe 5/10; Provides Ezetimibe= 2.5 mg, Rosuvastatin 1.25 mg
-Day four: 1/4 pill of Rosuvastatin, provides 1.25 mg
-…same as above
According to literature, the above combo should provide a mean decrease of about 40-50% LDL.
By the way, presently I take no pharmaceutical drugs and my non-HDL cholesterol (the best ApoB proxy) is 122 mg/dL, a viable level (130 is the threshold indicated by Tom DAysprings in lack of other risk factors) but surely not optimal.
What I want to avoid is an increase in fasting blood glucose and that’s the main reason for statin minidosage.
1 Like
adssx
#997
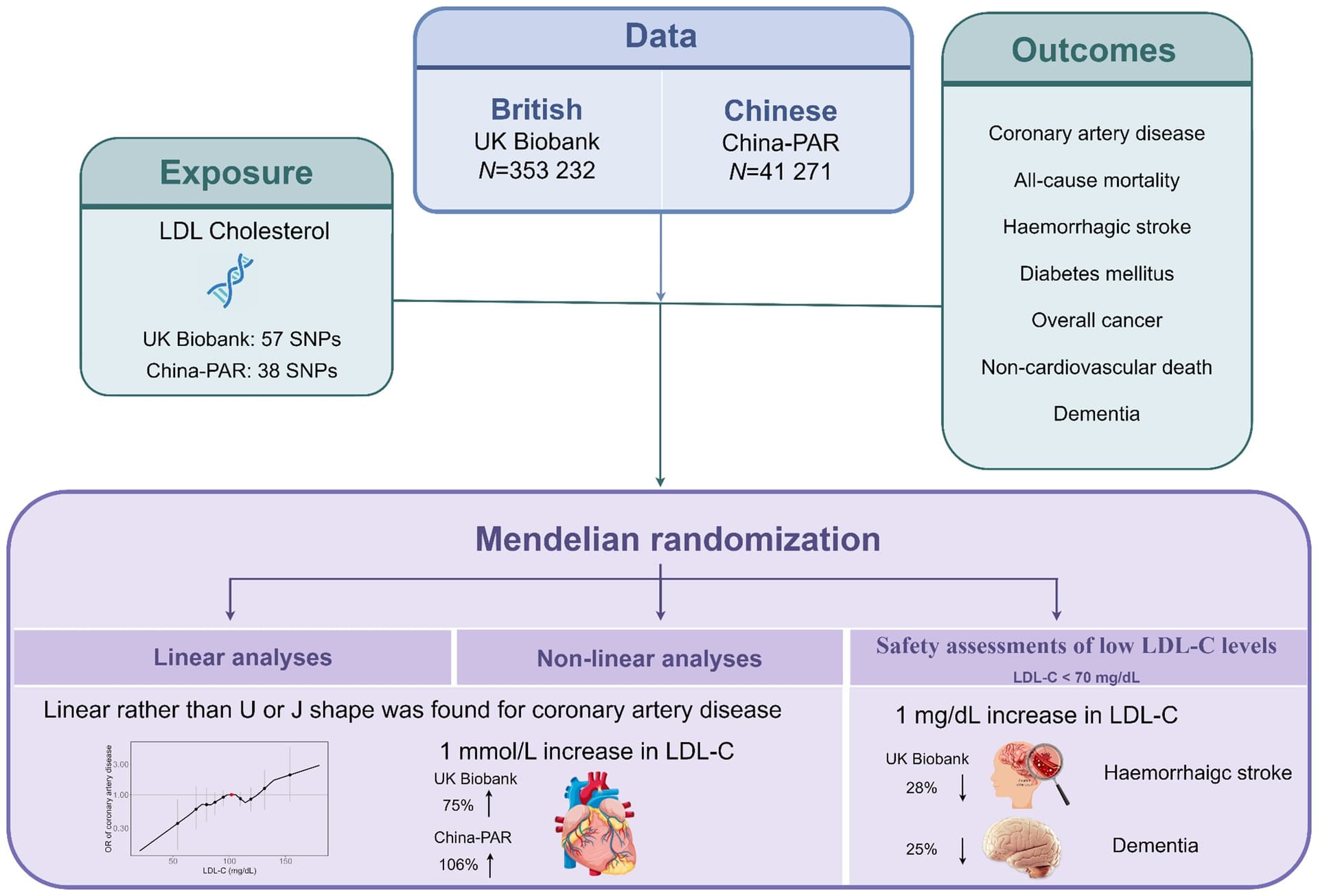
Efficacy and safety of low levels of low-density lipoprotein cholesterol: trans-ancestry linear and non-linear Mendelian randomization analyses 2023
Reposting this interesting study showing no lower threshold for LDL in terms of CAD risk reduction but a risk for dementia and stroke below 70 mg/dL. Does anyone have access to the whole article? I’d like to see the curve for stroke and dementia, is it flat above 70?
3 Likes
Both low and high levels of HDL-C were associated with elevated dementia risk. The association between LDL-C and dementia risk was modest.
https://www.neurology.org/doi/10.1212/WNL.0000000000207876
adssx
#999
That’s an association study. I cited a Mendelian randomization hinting at a causal link between low LDL and dementia.
1 Like
adssx
#1001
The one I posted is more recent and looks more serious given that Frontiers is not a great journal.
I think dementia is a tough nut to crack. There is a definite link for high LDL to dementia. Low LDL being linked to dementia seems a bit off.
I would assume that very low LDL levels mean one of two things: 1. The patient is diseased. Or 2. The patient is lowering their LDL in response to earlier detected high levels.
I think it’s very rare for individuals like us to proactively lower LDL without prior high LDL which may have started the dementia ball rolling.
1 Like