Dr. Greger hammers fishoil for CVD and ACM. Whatever happened to the omega index? I thought Dr. Greger took or recommended modest EPA/DHA supplementation for brain health, but maybe that’s changed:
2 Likes
RapMet
#1362
I’ve mentioned it before but for me fish oil (I used to take wild Norwegian cod liver oil) had absolutely no effect whatsoever in lowering my inflammation. Eating fish (wild caught) however does lower my inflammation quite a bit. so, I’m not sure if there are other substances in the fish which contribute to lowering inflammation (besides oil/fat), or if the oil in supplement form loses its effectiveness while being processed. Either way I stopped using fish oil after six months or so (with no effect) and try to eat fish once or twice weekly. I tend to get best results from colored ones (wild salmon or trout) as opposed to white fish (i.e. sea bass etc…).
2 Likes
What are you measuring in “inflammation?” I think Omega 3s are useful in reasonable amounts although as with many things moderation is a good idea.
I am not sure they help with reducing the levels of senescent cells, however.
3 Likes
RapMet
#1364
It is anecdotal but have an auto immune disorder and usually can tell immediately the effects of a substance or food. I also have King Charles  “fat finger” syndrome/condition (probably because of the autoimmune issue) and certain supplements and/or foods do reduce the inflammation on my hand and joints. Fish oil though didn’t have an effect. Obviously, it could still be beneficial for things other than inflammation though, but the usual claim that it fights inflammation didn’t seem to be the case with me.
“fat finger” syndrome/condition (probably because of the autoimmune issue) and certain supplements and/or foods do reduce the inflammation on my hand and joints. Fish oil though didn’t have an effect. Obviously, it could still be beneficial for things other than inflammation though, but the usual claim that it fights inflammation didn’t seem to be the case with me.
1 Like
I think the problem here is there are all sorts of things labelled as inflammation. They have different causes and need to be separately analysed.
5 Likes
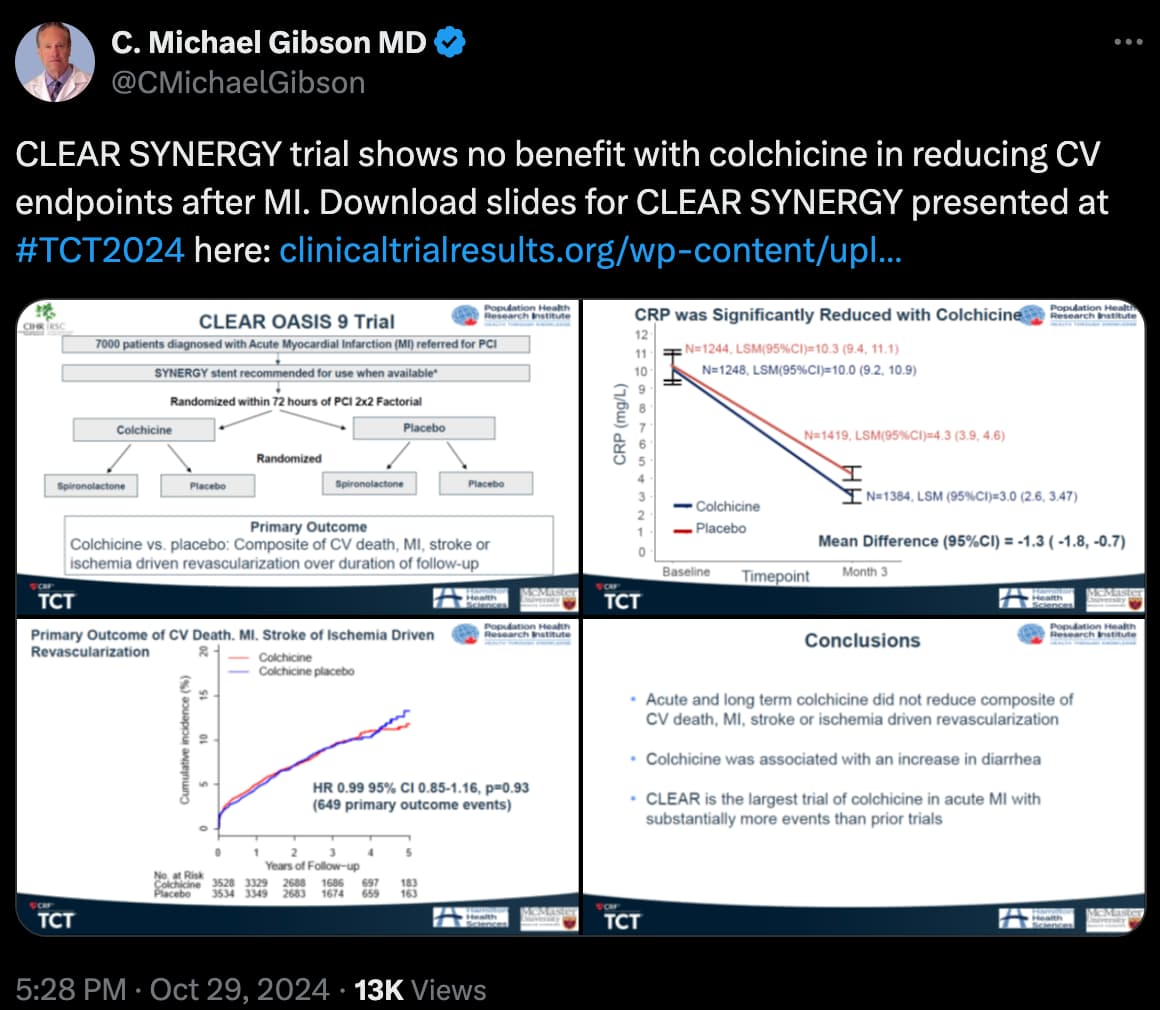
I think this puts the inflammation argument to bed (in regards to colchicine).
2 Likes
Or at least inflammation markers reduction mediated by colchicine.
2 Likes
Neo
#1369
I don’t know the trial - was it representative of all CVD?
There any many cases where one specific trial fails and the mechanism later is proven out in a powerful way and helps thousand of people
Is colchicine a complete representation of offset inflammation?
1 Like
Neo
#1370
See comment above, I don’t know the literature here - did a lot of other trials for other parts of CVD also show no results?
I think what you quoted contains the answer: as mediated by colchicine. It’s a comment on colchicine, not some other molecule and the possibility of some other molecule impacting inflammation and then in turn inflammation impacting CVD outcomes. Just colchicine. And furthermore, not even impact on inflammation, but on a particular inflammation biomarker. Think of it as a series of venn diagrams from the biggest to the smallest: CVD end points–>inflammation–>inflammation biomarkers–>inflammation biomarker–>colchicine. If colchicine only affects a given inflammatory biomarker, you don’t therefore assume that it must affect all inflammatory biomarkers (just the subset), and in turn, just because inflammatory marker(s) are affected doesn’t mean actual inflammatory processes are affected, and even if inflammatory processes are affected, doesn’t mean CVD end points must be affected. So as can be seen there are multiple leaps (steps) between colchicine and CVD outcomes, and a breakdown can occur at any of those steps, i.e. any of those steps can be a wrong assumption.
2 Likes
Yes, you guys are correct in that there are different types of inflammation. So, I should’ve probably said it puts the ‘colchicine and inflammation’ issue to bed in regards to CVD.
2 Likes
Does anyone remember the difference in ApoB and LDL lowering if you take 5 mg Atorvastatin every day vs EOD? Thanks in advance.
@A_User
adssx
#1374
Association of sodium-glucose cotransporter-2 inhibitor with regression of coronary plaque burden 2024
In the SGLT2i group, the non-calcified plaque burden [(39.86±14.30)% vs. (36.84±13.86)%, p=0.002)] and low attenuation non-calcified plaque burden (6.62 [4.11,10.13]% vs. 5.78 [3.40,9.28]%, p=0.042) were significantly decreased between two CCTA images. Whereas, in the non-SGLT2i group, there was no difference with regard to non-calcified and low attenuation non-calcified plaque burden between two CCTA images (all p>0.05). Moreover, changes of total plaque burden and non-calcified plaque burden were higher in the SGLT2i group than the non-SGLT2i group (all p<0.05). Importantly, SGLT2i was associated with total plaque volume (odd ratio=0.594, p=0.024) and non-calcified plaque volume regression (odd ratio=0.619, p=0.042) after adjusting for confounding factors.
SGLT2i significantly regresses coronary plaque burden, in particularly non-calcified plaque. These findings might explain the observed cardio-protective effect of SGLT2i in large trials.
8 Likes
Wow, Antoine, where the heck do you dig up these studies?! This one is a doozy. One thing always puzzled me, because I’ve read that SGLT2i can raise LDL levels, yet they were considered heart healthy. I just figured it must be some other non-lipid mechanism that was responsible for the heart protective effects of these drugs. Same way statins increase the calcification score (CAC), yet diminish MACE, because by calcifying the plaque they stabilize it and so it doesn’t rupture and cause blockages. But this study says the opposite, that SGLT2i can actually diminish plaque and they speculate that it is this that might be responsible for the heart protective effect. Very bizarre. How can you regress plaque while also raising LDL levels? I don’t get it. But hey I’m happy, as long as these results are real over the long term.
1 Like
adssx
#1376
I check ALL SGLT2i papers 
Yes but… not really. See: SGLT2-inhibition increases total, LDL, and HDL cholesterol and lowers triglycerides: Meta-analyses of 60 randomized trials, overall and by dose, ethnicity, and drug type 2024
Overall, changes were modest and not likely to be of clinical relevance.
Overall, using random effects models, SGLT2-inhibitor treatment increased total cholesterol by 0.09 mmol/L (95% CI: 0.06, 0.13), low-density lipoprotein (LDL) cholesterol by 0.08 mmol/L (0.05, 0.10), and high-density lipoprotein (HDL) cholesterol by 0.06 mmol/L (0.05, 0.07), while it reduced triglycerides by 0.10 mmol/L (0.06, 0.14).
For LDL, +0.08 mmol/L (0.05, 0.10) means… +3 mg/dL! So basically nothing.
6 Likes
OK, but they don’t lower LDL levels, so they must reduce plaque by some other mechanism than lowering LDL levels. But plaque regression in studies is always accomplished by lowering LDL, high intensity statins lower LDL, ezetemibe combos, PCSK9i lower LDL - that’s how all of them regress plaque, by lowering LDL. SGLT2i don’t lower LDL - so how do they reduce plaque? I start to wonder how real this result is.
1 Like
DrFraser
#1378
Vascular disease is multifaceted, but the low hanging fruit are:
Blood pressure, Insulin Sensitivity and Lipid optimization.
So minimally increasing LDL while lowering blood pressure and increasing insulin sensitivity, like occurs with the SGLT2-i on balance gives benefit. Also, I’d guess most individuals on one of these drugs is managing/optimizing their lipids anyway.
Here’s what Vera-Health.ai says on SGLT2-i and insulin sensitivity and BP.
SGLT2 inhibitors, primarily used for managing type 2 diabetes mellitus (T2DM), have been shown to both lower blood pressure and increase insulin sensitivity, offering benefits beyond glucose control.
Blood Pressure Lowering: SGLT2 inhibitors have a significant blood pressure-lowering effect, which is dose-independent and comparable to low-dose hydrochlorothiazide 2. This effect is primarily due to natriuresis and osmotic diuresis, which reduce blood volume and subsequently lower blood pressure 9. Additionally, these drugs improve vascular function by reducing oxidative stress and inflammation, further contributing to their blood pressure-lowering effects 4.
Insulin Sensitivity: SGLT2 inhibitors have shown potential in improving insulin sensitivity. For instance, empagliflozin has been demonstrated to improve hypothalamic insulin sensitivity in patients with prediabetes, suggesting a potential reversal of brain insulin resistance 1. The mechanism involves reducing glucose reabsorption in the kidneys, leading to glucosuria and a decrease in blood glucose levels 1. This reduction in glucose levels can improve insulin sensitivity by decreasing the need for insulin secretion and improving β-cell function. Furthermore, SGLT2 inhibitors promote weight loss and modulate adipocyte function, which also enhances insulin sensitivity 1.
In summary, SGLT2 inhibitors effectively lower blood pressure through mechanisms involving natriuresis and vascular improvements, while also showing potential to enhance insulin sensitivity by modulating glucose levels and adipocyte function. These effects make SGLT2 inhibitors a valuable therapeutic option for managing T2DM and its associated comorbidities.
4 Likes
OK, so if you already have low/optimal BP, and have good insulin sensitivity and glucose levels, SGLT2i are useless /jk/
2 Likes
adssx
#1380
It’s just one Chinese paper (but from a good uni and in a good journal) so it might be incorrect. However another paper suggests the same thing (at least in diabetic mice, a you say for those with “low/optimal BP, and have good insulin sensitivity”: no one knows): Glucose lowering by SGLT2-inhibitor empagliflozin accelerates atherosclerosis regression in hyperglycemic STZ-diabetic mice
4 Likes