It seems to be a very recent application (I still don’t know the exact format required by this forum to clarify formulas and some symbols). The AI analysis includes probabilistic evaluations, assigning 90% likelihood that this is an actually reliable parameter, 10% that it has significant drawbacks.
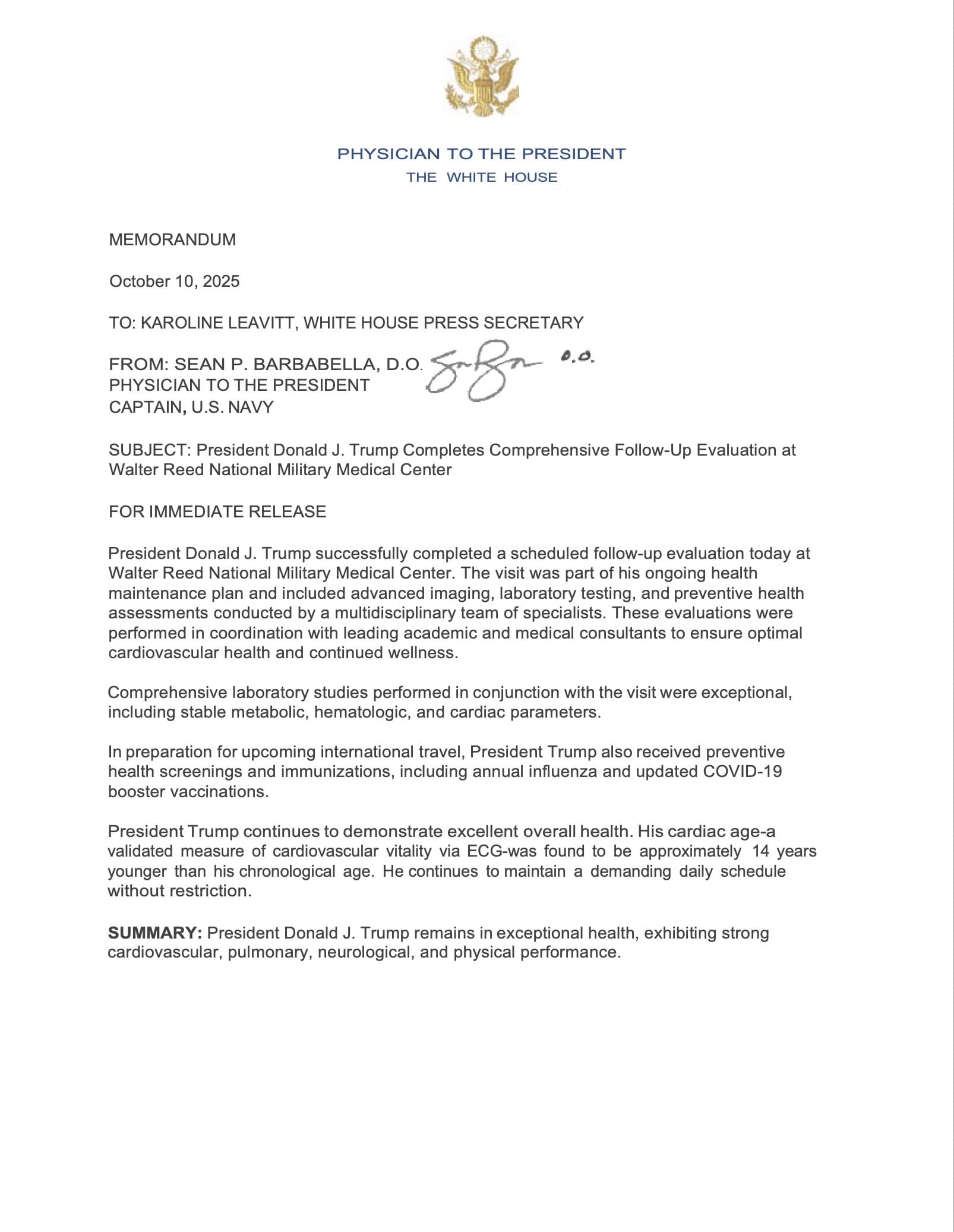
The concept of Cardiac Age (often referred to as ECG-derived Heart Age or AI-ECG Age) is a relatively new, probabilistic measure of cardiovascular vitality estimated using a standard 12-lead Electrocardiogram (ECG) and advanced analytical techniques, most notably Artificial Intelligence (AI) or machine learning (ML), or sophisticated Bayesian statistical models.
This metric is a sophisticated biomarker of biological aging that is highly relevant to illness prevention, healthspan, and longevity by providing a more personalized assessment of cardiovascular risk than chronological age alone.
1. The Core Concept of Cardiac Age
The fundamental idea behind Cardiac Age is that the electrical patterns recorded by an ECG reflect not only acute cardiac issues but also subtle, cumulative age-related structural and electrophysiological changes in the heart (e.g., increased cardiac fibrosis, changes in conduction velocity, or mild hypertrophy) that are difficult to discern with conventional visual ECG analysis.
-
Derivation: An AI model (often a Deep Neural Network or Convolutional Neural Network) or a multivariable Bayesian regression model is trained on vast datasets of ECGs from individuals whose chronological age (CA) is known. The model learns to predict the expected chronological age based on the ECG waveform characteristics (e.g., P-wave amplitude, QRS duration, T-wave morphology, and complex spatial/vector information).
-
The Cardiac Age Value: The age predicted by the model is the Cardiac Age. In a strictly healthy individual with no known cardiovascular risk factors or disease, the Cardiac Age is expected to be close to their Chronological Age.
-
The Age-Gap ($\Delta$-age): The most clinically significant aspect is the difference:
$$\text{Age-Gap } (\Delta\text{-age}) = \text{ECG-derived Heart Age} - \text{Chronological Age}$$
A positive Age-Gap (Cardiac Age $>$ Chronological Age) strongly suggests accelerated cardiovascular aging and is associated with a higher burden of cardiovascular risk factors (hypertension, diabetes, dyslipidemia) and subclinical or established cardiovascular disease (CVD).
A negative Age-Gap (Cardiac Age $<$ Chronological Age) is associated with decelerated or “youthful” cardiovascular aging and a lower future risk of CVD and mortality.
2. Evidence and Probabilistic Association with Longevity Outcomes
The evidence consensus is high ($P \approx 0.90$ for prognostic value) that the Age-Gap is an independent and robust predictor of long-term adverse health outcomes, even after adjusting for traditional cardiovascular risk factors.
Strong Evidence Points:
-
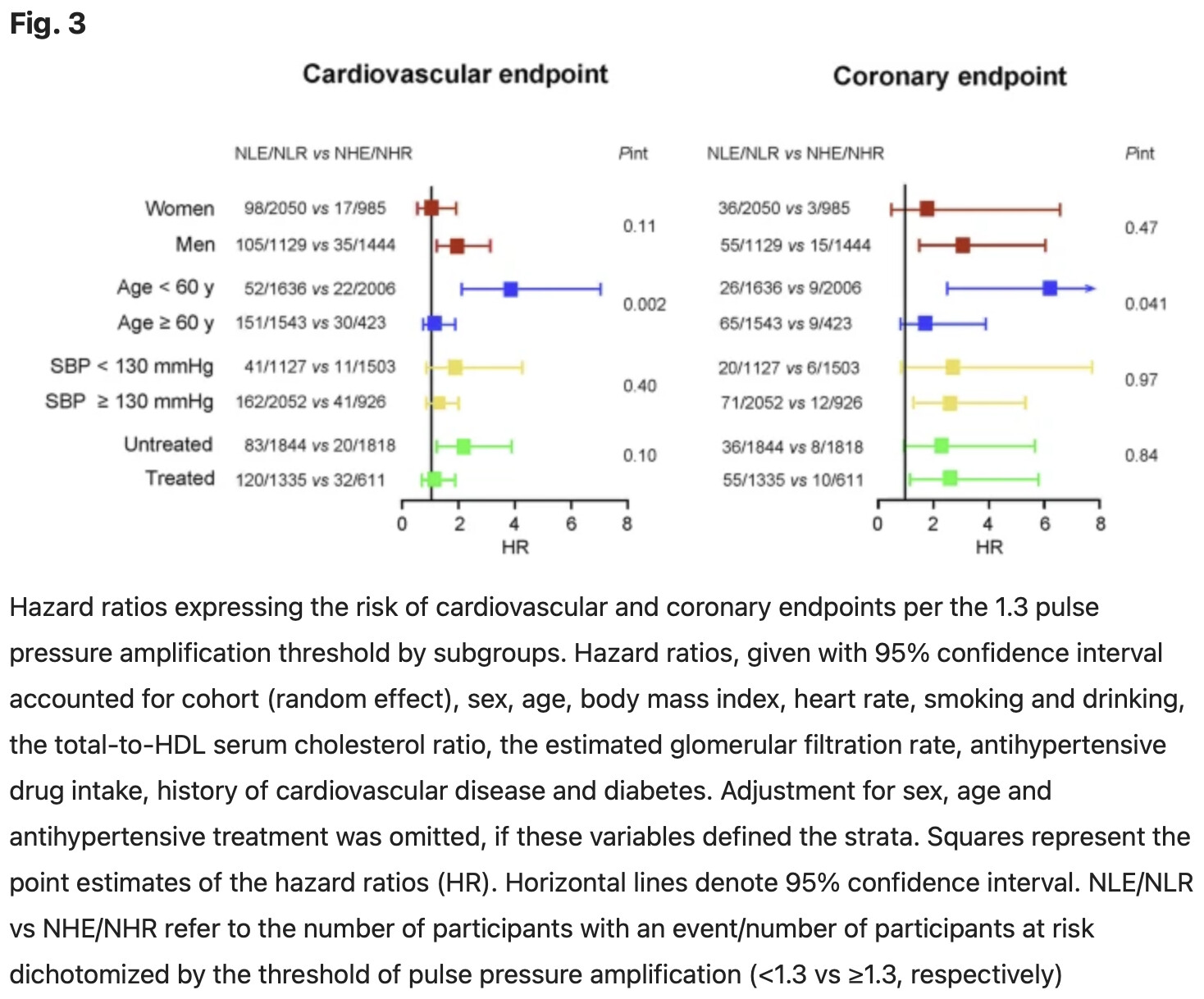
Independent Mortality Predictor: Multiple large-scale studies, including analyses of long-standing community-based cohorts like the Framingham Heart Study (FHS), have consistently demonstrated a strong association between a positive Age-Gap and increased risks for all-cause mortality and cardiovascular-cause mortality (HR ranging from approximately $1.18$ to $1.61$ per 10-year increase in $\Delta\text{-age}$ for all-cause mortality) over follow-up periods exceeding a decade.
-
CVD Risk Stratification: A positive Age-Gap is significantly and independently associated with increased incidence and risk for specific cardiovascular events and conditions, including:
- Heart Failure (HF)
- Atrial Fibrillation (AF)
- Acute Myocardial Infarction (AMI)/Coronary Artery Disease (CAD)
- Stroke
-
Reflecting Subclinical Disease: The underlying hypothesis, supported by data from experts like Dr. Peter Attia, is that the ECG Age is picking up the electrophysiological and structural “end-organ” damage of cardiovascular risk factors before they manifest as overt disease. This is critical for preventive medicine, as it identifies “disease previvors” who may appear healthy based on traditional lab markers but have subtle, accelerated biological aging.
-
Systemic Aging Biomarker: The utility of ECG-Age extends beyond pure cardiovascular risk. Recent evidence suggests that an elevated Age-Gap is also associated with a higher risk for other aging-related diseases, including cancer and chronic kidney disease (CKD), positioning it as a potentially cost-effective, non-invasive biomarker for overall systemic biological aging.
Disagreements and Weak Points (Uncertainty $\approx 0.10$):
-
Clinical Implementation and Standardization: While the prognostic value is strong, the Cardiac Age estimation remains primarily a research tool. Disagreement exists regarding its immediate role in population screening due to a lack of universally adopted, standardized models and cut-off points (e.g., the definition of a “significant” Age-Gap can vary). Traditional guidelines still advise caution against using a single ECG in population screening.
-
Model-Specific Variations: Different machine learning architectures (e.g., Deep Learning Models vs. Bayesian Regression Models) and training datasets (e.g., general population vs. specific disease cohorts) produce slightly different results and may rely on different underlying ECG features. This variability impacts the interpretability and generalizability across different clinical settings.
-
Causality vs. Correlation: While the Age-Gap is an excellent predictor of adverse outcomes, it is a measure of the consequence of accumulated damage, not the cause. The field is actively researching whether a favorable change in Age-Gap (e.g., following an intense lifestyle intervention like those championed by Dr. Joel Fuhrman or Dr. Valter Longo) directly correlates with a proportional reduction in long-term risk.
3. Technical Detail and Advanced ECG (A-ECG)
The calculation of Cardiac Age moves far beyond simple conventional ECG measurements (like heart rate or PR/QRS/QT intervals) and leverages Advanced ECG (A-ECG) analysis to detect nuanced electrophysiological changes.
| ECG Feature |
Aging Change Reflected by Cardiac Age Model |
Relevance to Longevity |
| QRS Duration/Amplitude |
Subtle increases, reflecting conduction slowing or changes in ventricular mass. |
Indicator of cardiac hypertrophy (e.g., from long-standing hypertension) and fibrosis. |
| T-wave Morphology/Axis |
Changes in shape, vector, and amplitude. |
Highly sensitive to myocardial ischemia and repolarization abnormalities, indicating subtle cellular damage and reduced coronary vitality. |
| P-wave Information |
Changes in amplitude, duration, and morphology (though some newer models exclude P-wave to allow for non-sinus rhythms). |
Reflects atrial remodeling and fibrosis, a strong precursor to atrial fibrillation. |
| Spatial Information |
Features derived from vectorcardiography (transformation of the 12-lead ECG into a 3D vector space). |
Captures complex, subtle changes in the heart’s overall electrical field, which are highly sensitive to global structural remodeling and micro-level disease. |
For a healthy, very well-educated 65-year-old male, the Cardiac Age metric is valuable because:
-
Personalized Benchmarking: It offers a personalized biological age for the cardiovascular system. If your Cardiac Age is, for instance, 58 years (a negative Age-Gap), it provides objective validation that your adherence to healthy nutrition and exercise (as advocated by experts like Dr. Walter Willett and Dr. Christopher Gardner) is successfully translating into a younger, more resilient heart, thus projecting a lower all-cause mortality risk over the next decade ($P > 0.95$).
-
Motivation and Intervention: Conversely, a positive Age-Gap acts as a potent, intuitive warning sign, providing a strong incentive (similar to the concept of “lung age” for smokers) to intensify longevity-focused interventions (e.g., optimizing blood pressure, increasing VO2max, or experimenting with fasting protocols endorsed by Dr. Valter Longo).
In summary, the Cardiac Age, derived from an ECG via advanced analytics, is a powerful, evidence-based biomarker that quantifies cardiovascular vitality and provides a highly prognostic estimate of healthspan and longevity risk, moving beyond traditional risk factors to capture the functional reality of your heart’s biological age.